Ep 14 – Ketamine for the FRCA
17 November 2024
Contents
This episode is going to explore Ketamine and the knowledge you need for the FRCA primary.
Chiefly, its properties, clinical uses, metabolism / clearance and we will spend some time on the NMDA receptor complex and what it gets up to!
I want to stress right now that it is not a ‘get out of a corner in a dodgy hypotensive patient who needs an anaesthetic’ free card.
It will drop blood pressure in a patient who has spaffed all their catecholamines up the wall. Because it is a direct myocardial depressant too.
What is Ketamine?
Ketamine is a dissociative anaesthetic that acts as an NMDA receptor antagonist. It provides analgesia and amnesia while maintaining airway reflexes and cardiovascular stability.
The NMDA Receptor
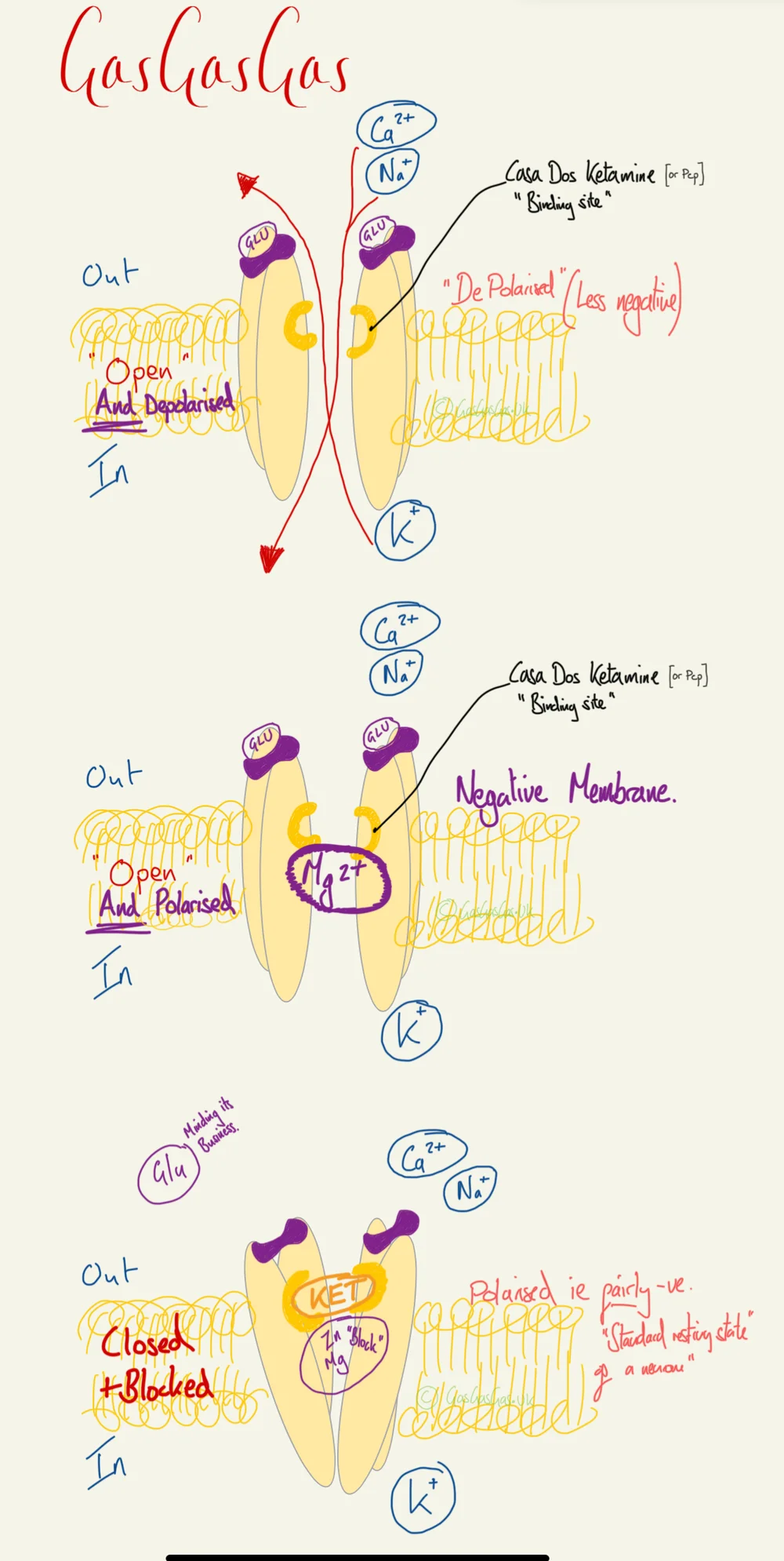
The NMDA (N-Methyl-D-Aspartate) receptor is a ligand-gated ion channel permeable primarily to Ca²⁺, found throughout brain and spinal cord. It requires simultaneous glutamate binding and membrane depolarisation to relieve Mg²⁺ block and enter an open state, making it central to synaptic plasticity, nociception, and anaesthetic drug targets.
-
NMDA: N-Methyl-D-Aspartate a chemical specific to the NMDA receptors binding site for it, it is not glutamate.
-
Found throughout brain and spinal cord
-
Transmembrane receptor
-
Ion channel for Ca mostly but any cation will make it in or out (when its in open state)
-
Made up of NR1 and NR2 subunits
-
Binding sites include Glutamate sites, NMDA sites, glycine and possibly several others.
-
These binding sites allosterically modify the receptor and may shift it into an ‘open’ state.
-
However the pore often ends up obstructed by magnesium despite being ‘open’
-
The magnesium is lurking there quite happily whilst the neurone is chilling in its hyper polarised resting negative state.
-
When a neurone is in a depolarised state this Mg2+ is displaced and only then will the activated NMDA receptor complex allow ion movement, rapidly being re-obstructed on return to resting membrane potential state.
-
The calcium influx is considered the probable mechanism by which the NMDA receptor mediates its physiological functions of neuronal plasticity, learning and memory formation.
-
Down stream effects of NMDA receptor port cation transit, (which is really really getting into the minutiae) lead to activation of NO synthetase causing nociception, probably central pain sensitisation and in extremes neurotoxicity.
-
The ketamine binding site, is also where PCP would bind, and is fairly close to where the Magnesium binding lurks
-
Ketamine blocks the channel, but also in allosteric terms modifies the complex and reduces the time the channel can be in its open state.
Core Concept
Ketamine is a phencyclidine derivative supplied as a racemic mixture of S- and R-enantiomers; esketamine (S-ketamine) is 2–4× more potent than R-ketamine and is associated with fewer emergence effects at equivalent doses.
Name - Ketamine
- Class: Phencyclidine Derivative
- Colour / appearance: Clear colourless liquid
- Additive: Benzethonium Chloride
- Preparation : A racemic (50:50) mix of S (good) and R Ketamine (baddy) enantiomeric mix
- Concentration: often provided at 50mcgs/ml or ampoules of 100, 250, 500mg as a powder (reconstituted in saline)
- Esketamine is 2-4x the potency of R-Ketamine
Dose Route
Chiefly IV or IM, There is an oral preparation also. - Note that dosing of ketamine is quite spectral - with a little bit maybe helping with pain - but also making folks feel quite strange sometimes a lot certainly anaesthetising/sedating - but a middle ground may yield a lot of paranoia and ‘strange’ with little benefit.
Anaesthetic Dosing
| Route of Administration | Dose | Onset Time | Length of Anaesthesia |
| IV | 0.5 -2mg/kg | 30-90s onset | 5-10 min of anaesthesia |
| IM | 4-10mg/kg | 2-8 min onset | 10-20 mins of anaesthesia. |
| IV anaesthetic maintenance | 10-50 micrograms / min |
Ed 95 for anaesthesia 1.3mg/kg
Sedating and Analgesic
| Route of administration | Dose | Onset Time | Length of Anaesthesia |
| IM Sedating Dose | 2-4. mg/g. (some say 3-4mg/kg | 2-8 Mins | |
| IV Sedating Dose | 0.2-0.75 | 30s+ | |
| Ketamine Pain Dose | 0.1-0.5mg/kg | 30s + | 4+ hours apparently. |
Pharmacodynamics of Ketamine
Mechanism of Action of Ketamine
- NMDA Receptor: Non-Competitive NMDA antagonist,
- OPIATE Receptor: SKET fancies itself as an 4x potency opioid receptor agonist relative to RKET
- MUSCARINIC Receptor: Perhaps how its broncho dilating effects and sialorrhea effects are caused
- Sodium channel blockade: technically can be a local anaesthetic. Experimentally used for regional, is neurotoxic
Side effects of Ketamine
Ketamine’s side-effect profile reflects its sympathomimetic action, NMDA antagonism, and direct myocardial depression, spanning cardiovascular, respiratory, neurological, ocular, and metabolic systems.
CVS
- HR / BP / SVR increase with sympathomimetic effect mediated by inhibiting neuronal reuptake of nADR.
- BUT has direct myocardial depressant activity
- Profound hypotension in ‘catecholamine deplete states’ R-Ketamine is more of the baddy here.
Respiratory
- Increased Respiratory rate
- Bronchodilating
- Preserves airway reflexes but causes
- Hypersalivation!
- Reduces PVR
Neuro
- Eyes open
- Mydriasis
- Nystagmus
- Emergence delirium,
- ICP increase
Nowadays considered appropriate in the head injured neuro patient as hypotension significantly larger issue. While studies in animals find neuroprotective benefits, this has never borne out in humans. It is probably not good for neonatal/infant brains
Eyes
Increase IOP (not for those ruptured globe anaesthetics!)
Metabolic
Metabolites in chronic exposure likely injurious to bladder.
Pharmacokinetics of Ketamine
Ketamine has a pKa of 7.5 (~44% unionised at physiological pH), a volume of distribution of 3 L/kg, undergoes hepatic N-demethylation to nor-ketamine (30% activity), and has a terminal half-life of 2.5 hours.
Absorption
- 20-25% bioavailability on oral ingestion
Distribution
- pKa 7.5 → ~44% unionised at pH 7.4 (≈56% ionised)
- Henderson–Hasselbalch for a weak base: % unionised = 100 ÷ (1 + 10^(pKa − pH)) = 100 ÷ (1 + 10^(7.5 − 7.4)) = 100 ÷ (1 + 10^0.1) = 100 ÷ 2.259 ≈ 44%
- Caveat: ketamine’s unionised fraction is sparsely documented — standard texts quote the pKa (7.5) but seldom the derived percentage. The 44% here is calculated from that pKa; a few sources cite a lower pKa (~7.2), which would push the unionised fraction toward 60%, so treat the exact figure as approximate.
- VOD 3 litres
- Protein binding : 20-50% protein bound (least of the hypnotics)
- Apparently more lipid soluble than thiopentone according to a BJA ed article
Metabolism -
Liver
N-demethylation producing Nor-ketamine which has 30% activity and subsequent hydroxylation or conjugation into water soluble molecules that are cleared renally
Elimination
Clearance 17ml/kg/min
Redistribution Half-life 11 mins
Terminal Half-life 2.5 hours
Define or Die
What Are Enantiomers?
Always forget this one, so ive broke the word down courtesy of the internet
Enantios means opposite,
Mer, Meros, means partIn our realm it talks about a molecule with a chiral centre that carries a conformation change around that centre, ie, same molecules, different layout, that when split into their respective groups rotate polarised light in a particular direction.
Bupivacaine, adrenaline, etomidate, ketamine, tramadol are all enantiomers
Check out the Classifying isomers episode to get to grips with this core concept!
Disassociated Anaesthesia
Ketamine induces this state, described as a thalamo-cortical disconnect, I think of it as the brain is “on”, but isn’t getting any external stimulus, leads to quite an active EEG.
Clinical Relevance
Ketamine’s most clinically significant caveat is haemodynamic: in catecholamine-depleted patients its direct myocardial depression predominates over sympathomimetic stimulation, causing hypotension.
-
Takes a while to work and then end point is pretty vague but generally the patient is rendered unresponsive and glazed, they might not shut their eyes, which can be weird.
-
Having spoken with a naval anaesthetist who worked in Afghanistan, they sometimes dosed down to 0.25mg/kg body weight for induction,
-
It definitely does drop BP in someone who is very sick and hasn’t got much in the way of catecholamines left to release into their SNS.
-
Useful for sedation in resus, to pull bones/joints into better alignment, lasts a while but then so does propofol before you can deem them ‘recovered’
-
Reached for in ITU for severely bronchospastic patients on the vent, and a good choice for that 50p20p Asthma RSI (but does cause sialorrhea!)
-
A fairly good IM you’ve been very naughty and your going to have a GA now despite no IV access drug, but does retain the need to get near enough to the patient to jab them in the leg/bum, and takes a fair while (10 mins) to work.
-
S-ket and R-ket at equal plasma conc have same delirium effects, but as esket is more potent, you give a smaller dose = less issues
-
Onset can be seemingly very rapid, patients quite quickly experience a ‘glazing over’ seem to make the odd sounds or brief few words and then the lights are out, I have seen one geology professor (doing coastal geology of course) describe an outer bodily experience whilst having his snapped femur straightened out, describing seeing us from above pulling on his leg, he said ‘oww that hurt’ as they pulled, and then reflected that ‘oh that didn’t hurt, how very strange…
In summary
It’s an ace drug for if you aren’t waking them up immediately afterwards , but isn’t used for routine operating given its psychosis flavoured emergence delirium/paranoia.
Reached for in ED because it is perhaps safer than propofol for sedation to pull limbs etc.
Next episode is a bit more parochial and is going to explore morphine in a similar manner
References
Jewett BE, Thapa B. Physiology, NMDA Receptor. [Updated 2022 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519495/
Anirudda Pai, Mark Heining, Ketamine, Continuing Education in Anaesthesia Critical Care & Pain, Volume 7, Issue 2, April 2007, Pages 59-63, https://doi.org/10.1093/bjaceaccp/mkm008
Laetitia Mony, Pierre Paoletti, Mechanisms of NMDA receptor regulation,Current Opinion in Neurobiology,Volume 83,2023,102815,https://doi.org/10.1016/j.conb.2023.102815.
Jürgen Schüttler, Helmut Schwilden, Handbook of Experimental Pharmacology Modern Anesthetics, Springer Berling, Heidelberg, 1stedition, 2008
Common questions
What is dissociative anaesthesia?
Dissociative anaesthesia is a drug-induced state of thalamo-cortical disconnection in which the patient is unresponsive to external stimuli but retains an active EEG. Ketamine produces this state via non-competitive NMDA receptor antagonism. Unlike conventional general anaesthesia, airway reflexes are largely preserved and cardiovascular tone is [mostly] maintained through sympathomimetic stimulation.
How does ketamine act at the NMDA receptor?
Ketamine enters the NMDA receptor channel and blocks it in a non-competitive manner, reducing the time the channel spends in its open state. The receptor normally requires simultaneous glutamate binding and membrane depolarisation to displace its Mg²⁺ block; ketamine binds near the magnesium site within the open channel pore, inhibiting Ca²⁺ influx and downstream nociceptive signalling.
Why can ketamine cause hypotension in critically ill patients?
Ketamine is both a sympathomimetic and a direct myocardial depressant. In euvolaemic patients, sympathomimetic stimulation predominates, raising heart rate, blood pressure, and SVR. In catecholamine-depleted patients — for example in haemorrhagic shock or the later stages of sepsis — endogenous stores are exhausted and the direct myocardial depressant effect is unmasked, causing profound hypotension.
What are the main pharmacokinetic parameters of ketamine?
Ketamine has a pKa of 7.5 (approximately 44% unionised at physiological pH by Henderson–Hasselbalch), a volume of distribution of 3 L/kg, and protein binding of 20–50%. It undergoes hepatic N-demethylation to nor-ketamine, an active metabolite with 30% of parent drug activity. The redistribution half-life is 11 minutes and the terminal half-life is 2.5 hours.
What is esketamine and how does its potency compare with racemic ketamine?
Esketamine is the S-enantiomer of ketamine, available as a purified preparation. It is 2–4 times more potent than the R-enantiomer at the NMDA receptor. Because an effective anaesthetic dose of esketamine is therefore smaller, emergence delirium and psychotomimetic effects are reduced compared with an equianaesthetic dose of the racemic mixture.
Thanks for listening. Take it day by day, don't overcook yourself — keep studying.
Transcript
14 min listenRead the full transcript
Introduction and Podcast Overview
00:00-00:58
Please listen carefully. Hello and welcome to Gas, Gas, Gas, your one-stop podcast for the FRCA primary exam. This podcast will fill your brain with information. Listen to it, think about it, and check out the show notes on the website. There you will find the core diagrams you need to be able to draw and describe for the exam.
This podcast can squeeze into your day. Listen while you’re driving to work, cooking dinner, maybe when you’re on call, or in the gym. Eventually the revision is going to end, but for now expect facts, concepts, model answers and the odd tangent. Remember to rate and follow the show to hear much, much, much more.
Hello, my fellow Gas Gas collaborators. This is James from Gas Gas Gas and today we are talking everything you need to know about ketamine for the primary FRCA exam. We’re going to look at its properties, its clinical uses, and spend some time on the NMDA receptor and what that gets up to. We’re going to pile straight into some questions, because I think that’s probably the best way to cover this.
The NMDA Receptor: Structure and Function
00:59-03:23
Doctor, tell me about the NMDA receptor and its function in the human body.
Oh, yes, the NMDA receptor found throughout the brain and spinal cord. It is a transmembrane receptor made up of NR1 and NR2 subunits, and it is an ion channel, mostly for calcium, but other cations can transit it either in or out of a neuron. It has a number of additional binding sites which allosterically modulate its action.
Glutamate, NMDA, glycine, and a number of others are suggested to bind to it. Oh, I’ve just remembered I should have defined NMDA, shouldn’t I? Sorry, Examiner. NMDA stands for N-methyl-D-aspartate receptor.
This receptor is found on neurons. Even when it’s in its open state, if a number of these allosteric modulators have bound and conformationally changed it to be open, it is often obstructed by magnesium in a non-depolarised neuron, i.e. one in its resting state. This magnesium obstructs the flow of cations. Therefore it means that this obstructive magnesium ion is actually critical to the functional nature of this receptor.
In the resting state the neuron is relatively electronegative, and the positivity of a magnesium cation means that it sits quite merrily in this pore. It is only displaced when the neuron itself depolarises due to it receiving an action potential sufficient to trigger depolarisation.
When it meets these criteria and the pore is in fact open and unobstructed, calcium influx is the chief cation that shifts. However, sodium can also influx through this pore, and potassium can escape from the intracellular environment. The calcium influx is considered the probable mechanism by which the NMDA receptor mediates its physiological function.
These are neuronal plasticity, learning, and memory formation. It is also involved in the modulation of pain. Downstream effects of this calcium influx, which I’d be surprised you’re getting to if the examiners let you talk this far, is nitric oxide synthetase inducing nociception can cause neurotoxicity in significant amounts and is probably involved in some of that central pain sensitisation.
Hopefully the examiner has jumped in well before now and poses another question.
NMDA Receptor Antagonists
03:23-03:35
Ah, well, that’s all well and good. What drugs can you think of that interact with this NMDA receptor?
The chief drug that comes to mind here is ketamine.
Yes, yes. Tell me more about ketamine, please.
Ketamine: Presentation and Dosing
03:35-04:43
So ketamine is a phencyclidine derivative. It is presented as a clear colourless liquid in a racemic mix of S and R ketamine, often provided either in solution at fifty milligrams per mil, or ampoules of one hundred to two hundred and fifty, or five hundred milligrams, as a powder that needs to be reconstituted in saline.
Of note, regarding the racemic mix, S-ketamine is two to four times as potent as R-ketamine and generally has a more favourable side effect profile.
The dosing route for ketamine is chiefly IV or IM, although there is an oral preparation too. Dose-wise, depends on your end goal, be that anaesthesia or sedation or analgesia. IV general anaesthesia is achieved with a range of either 0.5 to 2 milligrams per kilo, depending on your patient and their clinical state. Onset time for that is thirty to ninety seconds, lasting for five to ten minutes.
For the sake of time, I’ll be nice and succinct with the doses. An IV analgesic dose is 0.1 to 0.5 milligrams per kilo. The IM doses are higher.
Pharmacodynamics and Mechanism of Action
04:43-05:22
So from a pharmacodynamics perspective, its mechanism is actually multiple. Chiefly, it is a non-competitive NMDA receptor antagonist, but it also has activity at the opioid receptor, the muscarinic receptors, and sodium channels on neurons. It generally produces a dissociated anaesthetic due to disconnect between thalamus and cortex.
From a side effects perspective, cardiovascularly considered very stable, causing an increase in heart rate and blood pressure, mediated by inhibiting neuronal uptake of catecholamines in the sympathetic nervous system. It does have a direct myocardial depressant effect, though.
Respiratory and Other Effects
05:22-06:01
Ketamine preserves airway reflexes and maintains airway patency, significantly more so than other general anaesthetic agents. It increases respiratory rate, is a bronchodilator, but does cause hypersalivation. It’s also noted to reduce pulmonary vascular resistance.
It can increase intraocular pressure. Its other neuro effects include an increase in cerebral blood flow and intracranial pressure. However, this is not significant in the context of head injury generally.
It has a significant neurological side effect of emergence delirium, which can be significantly distressing for patients. That can be mitigated with midazolam.
Pharmacokinetics
06:01-06:47
From a kinetics perspective, its oral bioavailability is poor, at around seventeen percent. Its volume of distribution is three litres, and it is twenty percent protein bound, which is the least of the hypnotic agents. Its pKa is 7.5. Its unionised fraction is perhaps sixty percent.
It is metabolised in the liver by N-demethylation producing norketamine, which has about thirty percent of the activity of ketamine. This is subsequently either hydroxylated or conjugated into water soluble molecules that are cleared renally.
Its clearance is seventeen mils per kilo per minute, and it has a distribution half-life of around eleven minutes, 2.5 hours for a clearance half-life. For plasma, so it redistributes really quickly.
Processed EEG Effects
06:47-07:24
And what happens to a processed EEG if you administer ketamine?
If they’re asking you these sorts of questions, it’s probably to kill time. The processed EEG, when you give ketamine, goes nuts. You probably need to frame it along the lines of, for example, BIS index monitoring - your BIS number will go up. This isn’t that the patient is more aware, it is a reflection of the disordered neuronal activity that’s leading to the algorithm interpreting that as consciousness or an increased level of alertness, probably a better word to use.
Understanding Enantiomers
07:24-08:28
So we’ve talked quite a bit there about the properties of ketamine. I just wanted to touch on enantiomers, mainly because I always forget about enantiomers, so I’ve decided to break down the word enantiomer for you using the wonders of the internet because I did not do classics.
So, enantios in Greek means opposite and meros means part, so opposite parts. And this refers to the fact that an enantiomer is the same molecular makeup, i.e. the same molecules, but in a differing position that differs around a fixed chiral centre.
What they found is if they divvied up these racemic mixtures into their component two halves and then shined polarised light at them, it would rotate that polarised light in a particular manner depending on which half you are shining it through. And that’s what we’re talking about when we’re saying S-ketamine or R-ketamine or levobupivacaine.
Other drugs that are like this: bupivacaine, etomidate, tramadol.
Clinical Uses
08:28-09:43
Now on to the practical side of things. Where do we actually use ketamine? Generally, ITU flavoured RSIs and laparotomy flavoured RSIs, and you would be well justified in reaching for it in your patient with an expanding intracranial lesion, needing a nice thoughtful anaesthetic that doesn’t cause hypotension.
The important thing to bear in mind here is that it does drop blood pressure if your patient is incredibly clapped out, because the mechanism by which that increase in blood pressure is mediated is driven by inhibiting reuptake of catecholamines in your sympathetic nervous system. But if someone’s literally tipped off the cliff with a systolic of sixty or seventy, they don’t have much in the way of catecholamines left, so you give the drug a dose you think is right, and actually all you cause is myocardial depression.
Anecdotally, but there’s also a paper on it, doses down to 0.25 milligrams per kilo IV for induction have been used.
Its other chief use is sedation in recovery to pull bones and joints into better alignment. And also you can reach for it in your severely bronchospastic patient. Hopefully they’re already on ITU and hopefully they’re intubated because it’s a nice bronchodilator.
Severe Asthma and Emergency Use
09:43-10:13
And if you’re thinking that you’re in that fifty percent, twenty percent life-threatening asthma and you’re going to intubate them situation, which is terrifying, it’s probably a good choice there as well. It does cause hypersalivation though. Bear that in mind.
A use that doesn’t see much action in ITU, but I think A&Es have a tendency, is the “you’ve been a fairly naughty boy and you’re going to have some sedation now, whether or not you like it” because you’ve got nasal IV access. Here’s some ketamine IM.
Clinical Experience and Anecdote
10:13-11:07
My experience of ketamine is the onset does seem to be quite rapid in very sick people. They get glazed over, they might make an odd sound or say a couple of words, and then space out.
But I have seen, entertainingly and interestingly, a professor who had snapped his femur walking along some slightly slippery coastline doing some professorial stuff describe an out-of-body experience in A&E recovery when we were using ketamine to straighten out his leg. He was describing seeing us from above, being like, “oh, that looks wonky,” and then went, “ow,” when we pulled his leg. However, then he said, “oh, oh, actually, that didn’t hurt. Oh, how very strange.”
It’s very curious as to what sort of plane of anaesthesia or sedation he was in to explain these things to us. But I imagine his slightly scientific mind was trying to make sense of the situation and was exploring it. It was very interesting. Anyway, getting carried away.
Summary and Conclusion
11:07-11:55
In summary, it’s an ace drug, especially if you’re not going to be waking the patient up because you dodge the emergence delirium. The reason why it’s not used as a routine agent is because of that delirium. Pairs really nicely with rocuronium.
The next episode is going to be a bit more parochial, and we’re going to explore morphine in a similar manner. So, my name’s James, and you’ve been listening to Gas, Gas, Gas. Thank you very much.
If you found it useful or awful, please like and subscribe and rate the show. Definitely check out the show notes for those diagrams and the detail of this content. It is a bucket of content to get to grips with. Keep working at it and you will get better, faster and stronger. It is vital to keep your interest alive for the science that we’re covering and not overcook yourself. You will be amazed by what you know come exam day. Don’t freak out, keep studying.
Enjoyed this? Review on Apple Podcasts Rate on Spotify
Support the show Help keep the lights on SBA question bank @ Teach Me Anaesthetics