Ep 1 – Rocuronium For The FRCA Primary
8 November 2024
Contents
The first ever episode of Gas Gas Gas, which looking back a year or so later, it has been quite a journey of technical and organisational progress, anyway, sentimentality aside.
We begin with Rocuronium, We talk pharmacologic data, mechanism of action and the neuromuscular junction.
We crack out a model answer of the ‘classic approach’ to answering a what is drug X? Type questions.
Roc (rocuronium) is a commonly used muscle relaxant, convenient because it is rapidly reversible with sugammadex (16mg/kg for RSI dose reversal)or, when you’ve a few muscle twitches, it can be nudged towards a return of muscle power with cheaper drugs. It is pretty stable from a side effect profile perspective, but does trigger anaphylaxis sometimes.
Model Answer for Rocuronium
The table below maps every pharmacology domain for rocuronium — class, mechanism, kinetics, dosing, and reversal — in the format expected for an FRCA Primary viva answer.
| Name | Rocuronium (Rapid-Onset-Curonium)! |
| Class | AminoSteroid – structurally related to [vecuronium](/episode/vecuronium/) |
| Stem | Desacetoxy analogue of vecuronium – (is considered a quaternary ammonium compound and hence not crossing BBB and Placenta) |
| History | Rocuronium introduced in 1994, trade names of rocuronium included Esmeron and Zemuron! 6x less potent than vecuronium |
| Chemical Name | Rocuronium Bromide |
| Colour/Appearance | Clear colourless solution 10mg/ml of rocuronium bromide in 25 and 50mg ampoules |
| Molecular weight | 609g/mol (Roc bromide) |
| Structure | C32H53N2O4 |
| Solubility | Prefers watery realms to the buttery realms (water-soluble — lean body weight dosing applies in obesity; Vd 0.21–0.3 L/kg unchanged with high BMI). |
| Pharmaco-Dynamics of Rocuronium | |
| Mechanism of action | Competitive non- depolarising neuromuscular blockade. |
| Actions | Rocuronium acts by competive antagonism of Acetylcholine nicotinic (N2) receptors |
| Onset Time of Rocuronium | 60-90 Seconds, (1.2 vs 0.6mg respectively) |
| Offset Time of Rocuronium | 15-40 minutes to see one twitch return (dose/Prop/volatile dependent) Progressively more prolonged with age >70 Extended with Hypothermia |
| Dose for Rocuronium | 0.6mg/kg intubating dose on paper @75 kg is 45mg. 80% ready for ETT at 60s. 20-40min Recovery Time Modified RSI = 1-1.2mg/kg = 75-90mg. 93-96% ready for a tube at 60 seconds. 1 hour recovery time Subsequent 0.15mg doses @75 = 11.25mg Infusion rate of 300-600 mics/kg/ hour. 22.5 – 45mg/hour – relatively non cumulative Note, v small infants, with immature NMJs are more sensitive. |
| Side effects | CVS: Mild vagolysis can raise HR and MAP Insignificant histamine release Resp: Rarely bronchospasm MSK/Neuro: Paralysis…. Anaphylaxis Other Pain on injection – stings like heck |
| Pharmaco-Kinetics of Rocuronium | |
| Absorption | No one seems to eat it… |
| Distribution | 30% protein bound Volume of Distribution 0.21-0.3 |
| Metabolism | Liver: 17-desacetyl-rocuronium (scant and minimal potency) Mostly processed through liver to bile Very Severe Liver dysfunction can result in accumulation as it doubles the half life of rocuronium |
| Elimination | Hepatic uptake and hepatobiliary excretion – 30-40% of dose is unchanged in bile Renal Excretion – a 10-20% unchanged urine Plasma clearance of 3.5-3.9 ml/kg/min Elimination Halflife is 66-80 mins |
| OTHER: | Suggamadex reversal… a gamma-cyclodextrin the doses for suggamadex are: 16mg/kr if you’ve just given an RSI dose 4mg /kg if you’ve a twitch 2mg/kg if you’ve a few twitches |
| Doest mix with thiopentone or dexamethasone, | |
| Stability | Lasts for 12 weeks out the fridge! so dont worry if its been on the side (although we all worry because we are type A folk) |
Molecule
Rocuronium bromide (C₃₂H₅₃BrN₂O₄, MW 609 g/mol) is a large, water-soluble aminosteroid — its bulk and quaternary nitrogen prevent BBB and placental crossing.
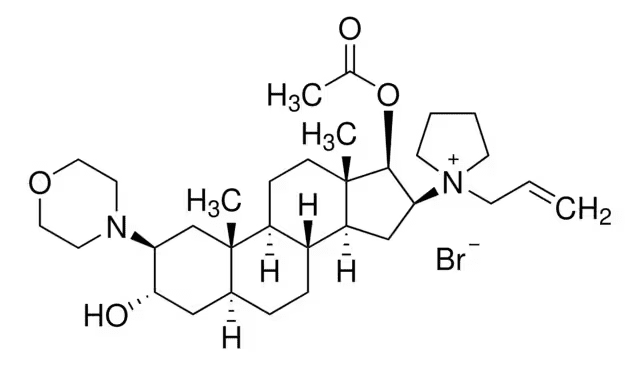
From Sigma Aldrich chemical data site – > direct link <
{kind=link}
As we can see, this is quite a big, complex molecule, in the context of anaesthesia agents at least.
Define or Die
Three terms are essential for answering any FRCA question on rocuronium or non-depolarising neuromuscular blockers.
- Non-depolarising – when given the muscles become flaccid without a disordered contractile process occurring first (unlike suxamethonium where the patient fasiculates)
- Competitive – the effects of rocuronium are reliant on there being sufficient concentration of the drug in the neuromuscular junction – so that it outcompetes acetylcholine
- Neuromuscular junction – NMJ, the interface between nerve and muscle which an action potential must cross.
Nicotinic Acetylcholine Receptors
Non-depolarising NMJ blockers are competitive antagonists of the nicotinic receptor at the neuromuscular junction.
When they bind to the receptor, they do not produce a conformational change (which may open the channel pore), but instead occupy the binding site and crowd out acetylcholine, which makes them competitive antagonists.
Their binding is transient and dynamic, with constant frequent association and dissociation of molecules, which means that acetylcholine and NMJ blockers are always fighting it out over the receptor.
Thus, increasing the concentration of NMJ blocker at the synapse gradually decreases the number of receptors available for binding acetylcholine, which gradually decreases the amplitude of the endplate potential.
Eventually, the endplate potential required to trigger depolarisation is so high that it does not reach the threshold required to activate the voltage-gated sodium channels, which means an action potential cannot propagate from Nerve to Muscle (triggering depolarisation of the muscle surface, Ca release from sarcoplasmic reticulum and all that fun)
Clinical Application
Used to paralyse practically every critical care patient requiring emergent rapid sequence induction (RSI), remember the dose is 1-1.2 mg/kg (Of Lean body mass)
Most people give 100mg, when modifying for high BMI the Society for Obesity and Bariatric Anaesthesia (SOBA) recommends lean body weight dosing, so it covers them too (Rocuronium is water soluble and doesn’t particularly like fat so it doesn’t influence its volume of distribution quite so much.)
In elective cases when used, the dose is 0.6mg.kg taking not as long as atracurium to work. Most people give less and wait longer before intubating. (the LD50 of rocuronium in rats is 0.3mg/kg so the art of waiting long enough with smaller doses before intubating is one to learn)
If you’ve just given suxamethonium or Rocuronium and then the sats trace disappears…. briefly think misplaced sats probe – and then think anaphylaxis.
The jury is neither in nor out for sugammadex to reverse anaphylaxis so that’s a choice for you, if you can suck a drug up that’s tickling mast cells, might be a good thing.
Roc is 6x less potent than vecuronium, so you give a higher dose. But because now you’re adding more competitive molecules…. Its onset is faster! (the Bowman Principle: low-potency agents require higher doses, steepening the plasma–NMJ concentration gradient and accelerating onset)
And also, some folks might be tempted to give a very small ‘pre-loading dose’ meaning they might reduce the MSK pains of their suxamethonium dose (pre-curarisation) or simply make their true ‘ intubating’ dose of agent work quicker.
Detailing the Neuromuscular Junction
For a comparative view of depolarising and non-depolarising block, see Paralysis, Suxamethonium, Rocuronium and Reversal.
The neuromuscular junction is a specialised synapse for the transmission of a signal from the motor nerve end plate/terminal bouton to a specialised postsynaptic region on the muscle cell surface.
Structure
- Presynaptic membrane
- Neuronal membrane featuring voltage-gated calcium channels and docked acetylcholine-filled vesicles that are ready for immediate exocytosis
- Synaptic gap
- Narrow (~70nm) space filled with basal lamina proteins and acetylcholinesterase
- Postsynaptic membrane (motor endplate)
- Deeply furrowed membrane, 8-10 times the surface area of the presynaptic membrane
- Covered in nicotinic acetylcholine receptors (10,000 per μm2).
Function
- An action potential arrives via the motor axon (100-120 m/s) (Alpha Motor Neurone)
- At the presynaptic membrane, voltage-gated calcium channels open in response to membrane depolarisation
- The intracellular calcium activates SNARE proteins which open acetylcholine vesicles
- Acetylcholine spills into the synapse (abundantly, with a safety factor of 3-5 times the minimum amount required to achieve endplate depolarisation)
- It is then rapidly (within 1ms) hydrolysed by a high-affinity acetylcholinesterase
- During its synaptic dwell time, acetylcholine activates nicotinic acetylcholine receptors
- These are pentameric ligand-gated transmembrane cation channels that mediate sodium entry into the cell
- The sodium influx depolarises the membrane and activates nearby voltage-gated sodium channels, creating the endplate action potential
- This action potential then propagates along the muscle fibre sarcolemma, notably delving into T tubules that penetrate deep into the myocyte where they activate calcium channels on sarcoplasmic reticulum necessary for excitation-contraction coupling.
- Presynaptic membrane – where vesicles are made and stored, that gets depolarised by the opening of sodium channels, which at the nerve terminal triggers calcium influx leading to a bunch of proteins getting activated (SNARE) which mobilise and fuse the vesicles.
A LOT of ACh gets launched into the cleft as it has to run a gauntlet of enzymes to make it to the nicotinic receptors on the other side
We will find ECF in the junction… and this reflects the plasma electrolyte state…. somewhat closely
Voltage-gated sodium channels in the skeletal muscle sarcolemma (muscle cell membrane) get activated, and the propagation of the action potential along this ends up going down T tubules. activating the contractile apparatus /the sarcoplasmic reticulum.
References
Khuenl-Brady, K.S., Sparr, H. Clinical Pharmacokinetics of Rocuronium Bromide. Clin-Pharmacokinet 31, 174–183 (1996). https://doi.org/10.2165/00003088-199631030-00002
Pharmacology of neuromuscular blocking drugs. BJA Education 2017. https://www.bjaed.org/article/S1472-2615(17)30002-X/fulltext
Society for Obesity and Bariatric Anaesthesia (SOBA UK). Lean body weight dosing guidance. https://www.sobauk.co.uk
Common questions
What is the intubating dose of rocuronium for RSI?
The modified RSI dose of rocuronium is 1–1.2 mg/kg (75–90 mg in a 75 kg patient), producing conditions suitable for intubation in 93–96% of patients at 60 seconds. Reversal requires sugammadex 16 mg/kg. The standard elective intubating dose is 0.6 mg/kg, with onset in 60–90 seconds.
How does rocuronium produce neuromuscular blockade?
Rocuronium is a competitive (non-depolarising) antagonist at nicotinic acetylcholine receptors (N2) at the neuromuscular junction. It occupies the receptor binding site without causing channel opening, crowding out acetylcholine. Blockade is concentration-dependent and reversible by increasing acetylcholine concentration or by sugammadex encapsulation.
Why does rocuronium have a faster onset than vecuronium despite being less potent?
Rocuronium is approximately 6–8 times less potent than vecuronium, so a higher molar dose is required for the same effect. This higher dose steepens the plasma-to-NMJ concentration gradient, accelerating diffusion to the receptor — the Bowman Principle. The result is onset of 60–90 seconds versus the slower onset of equipotent vecuronium doses.
How is rocuronium metabolised and eliminated?
Rocuronium undergoes minimal hepatic metabolism to the weakly active 17-desacetyl-rocuronium metabolite. The primary route of elimination is hepatobiliary excretion (30–40% of dose unchanged in bile), with 10–20% excreted unchanged in urine. Plasma clearance is 3.5–3.9 mL/kg/min and elimination half-life is 66–80 minutes. Severe hepatic dysfunction can double the half-life.
What are the main side effects of rocuronium?
Rocuronium causes mild vagolysis at higher doses, slightly raising heart rate and MAP. It produces insignificant histamine release compared with atracurium. Anaphylaxis is the most serious adverse effect — rocuronium is one of the commonest triggers of perioperative anaphylaxis. Pain on injection (particularly in the antecubital fossa) is a frequent complaint.
Thanks for listening. Take it day by day, don't overcook yourself — keep studying.
Transcript
13 min listenRead the full transcript
Rocuronium – Gas Gas Gas Podcast for FRCA Primary
Introduction and Podcast Overview
00:00-00:34
Please listen carefully. Hello, and welcome to Gas, Gas, Gas, your one-stop podcast for the FRCA primary exam. This podcast will fill your brain with information. Listen to it, think about it, and check out the show notes on the website. There you will find the core diagrams you need to be able to draw and describe for the exam. This podcast can squeeze into your day – listen while you’re driving to work, cooking dinner, maybe when you’re on call, or in the gym. Eventually, the revision is going to end, but for now, expect facts, concepts, model answers, and the odd tangent. Remember to rate and follow the show to hear much, much, much more.
Topic Introduction: Rocuronium Overview
00:34-01:22
Hello, and welcome to the inaugural podcast of Gas, Gas, Gas. Thanks for being here. The title of today is rocuronium. We’re going to quickly talk about when and where, going to go through a model answer, and then we’re going to talk about those delightful core concepts which are going to inform your paralysing agent choices. So, without further faffing, here we go.
So, rocuronium is a non-depolarising muscle relaxant. It’s commonly used and it’s exceedingly convenient. It’s rapidly reversible with sugammadex, or, towards the end of a case when it’s wearing off, you can nudge it towards normality with cheaper drugs than sugammadex, i.e., glycopyrrolate and neostigmine. Generally speaking, it’s stable from a side-effect perspective, but it does trigger anaphylaxis, and this is something to be aware of at induction.
Complete Model Answer: Rocuronium
01:22-02:58
So, Doctor, tell us about your favourite muscle relaxant.
“Oh, well, I really like suxamethonium.”
“Hang on. Hello. We want you to talk about rocuronium.”
“Oh, okay.”
So rocuronium is a commonly used non-depolarising competitive muscle relaxant of the aminosteroid class. It is often presented as a clear colourless solution in ampoules with a concentration of ten milligrams per mil. The dose is one to one point two milligrams per kilo in RSI, or zero point six milligrams per kilo for a standard induction dose during anaesthesia requiring intubation.
It’s considered structurally similar to vecuronium, although its onset time is quicker. The effect site it works at is the nicotinic cholinergic receptor in the neuromuscular junction found in skeletal muscle. It’s considered to be quite water soluble, is thirty percent protein bound and has a very low volume of distribution at zero point two seven litres per kilo.
“Shall I keep talking?”
“Yes, how is it cleared?”
So, rocuronium is eliminated chiefly by the liver, with a small amount excreted by the kidney unchanged. Therefore it would accumulate and would be slow to clear in patients with liver or renal disease.
Side effects of note: It is considered a mild vagolytic, leading to a transient rise in heart rate and blood pressure. It causes minimal histamine release, and very rarely causes bronchospasm. It is a known cause of anaphylaxis, and also of note: on IV injection it can sting and cause irritation.
“You’ve said a lot there, but what does rocuronium actually do?”
Rocuronium causes muscle paralysis. This is utilised in anaesthesia to facilitate intubation through vocal cords, which would relax and separate when a patient is sufficiently paralysed, but it also facilitates operative intervention where a body cavity needs to be accessed which paralysis may facilitate, such as laparoscopic surgery.
Key Terminology and Mechanisms
02:58-04:39
So I used a few terms there. Non-depolarising: rocuronium achieves its paralysis whilst not causing any depolarisation of the muscle, i.e., contraction. You might want to think about this as rocuronium leads to the muscle consuming less oxygen compared to other drugs, whereas, for example, suxamethonium causes widespread discoordinated contraction of the muscle motor units before flaccidity, and may consume more oxygen to do so. However, how relevant that is, is another question.
Competitive: rocuronium is competitive, i.e., if you were to introduce another agent to the neuromuscular junction that had an affinity for the nicotinic acetylcholine receptor, and you had ten rocuroniums and ten of this other drug, if they had an equal affinity, you would have a broadly equal degree of receptor occupancy with both of those agents. If you were to put a hundred rocuroniums in, then they would likely outcompete the other unknown agent. This is a concept that’s utilised for reversal.
The last term that came up there is the neuromuscular junction. We’ll go into this in great detail in another podcast, but this is the interface between neuron and muscle motor unit. It’s a very small cleft whereby depolarising signal from the nerve has to be transmitted to the muscle.
Clinical Practice and Dosing Strategies
04:39-06:51
But then let’s think about what we’re doing actually in reality with rocuronium. It’s all well and good, reeling off numbers like we give 1 to 1.2 milligrams per kilo in RSI, 0.6 milligrams per kilo for routine intubations. I’m sure you’ve all given more and given less, depending on the situation.
So, just to think about RSIs first. A rocuronium RSI used to give me the heebie-jeebies because I thought, “Gosh, they’re going to be very paralysed, and then I’ve got to go get some sugammadex and I’m going to feel pretty embarrassed and there’s a lot to think about and what if I can’t intubate them.” Hopefully, generally speaking, that anxiety is going to wane with time as you train. It has for me.
But if I was doing an RSI, I would generally give everyone one hundred milligrams because the situation at hand is they’re sick. You want to gain control. Paralysed patients are easier to ventilate if you needed to. And getting the tube in the hole is always a good thing because then you can focus on the hundred other tasks you need to deal with with a critically ill patient.
A hundred milligrams covers everyone. It even covers the morbidly obese. SOBA, which is the Society for Obesity and Bariatric Anaesthesia, recommend rocuronium targeted at lean body weight of an individual. So, therefore, everyone will end up sufficiently paralysed with a hundred milligrams, pretty much, unless you’re talking very, very, very muscular individual, in which case you might need to think twice and give them a bit more.
The things to remember when you’re thinking about this dose is it’s got very low volume of distribution, it’s very water soluble, so it doesn’t really get into the fat, so it doesn’t matter so much if they’re morbidly obese.
When you’re going down the route of in-theatre elective cases, some people prefer atracurium, some people like rocuronium, some people like rocuronium because you can bail out at the end and not think too hard about the dose if you just use sugammadex, which appears to be a tendency that’s slowly increasing as sugammadex is now cheaper.
Most people would probably give less rocuronium than 0.6 milligrams per kilo, and accept that they’ll have to wait longer to intubate. At the classic intubating dose, it’s one point five minute wait, whereas with atracurium at zero point five milligrams per kilo, you’re looking at about a three minute wait. So you might as well pick one you like or just mix and match as you see fit.
Critical Safety Considerations: Anaphylaxis
06:51-08:14
The important thing to never truly forget when it comes to rocuronium is it does cause anaphylaxis, and it causes anaphylaxis at entirely the wrong time, because you might think you’ve knocked their SATS probe off. You might think maybe I’ve intubated their oesophagus when I was rather sure that I was intubating the lungs. And sometimes when you’re getting someone off to sleep you get distracted. That three minute wait for paralysis to fully work with your atracurium or your one and a half with your rocuronium. You might start daydreaming or talking to the ODP. Bad news, don’t do that.
My experience was the SATS trace had disappeared and we were fiddling around with the SATS probe wondering why it wasn’t working before maybe about twenty seconds later we thought, “Oh, hang on, the SATS probe’s fine, and it’s just because there’s no pulsatile flow in their finger anymore because they’ve gone into florid anaphylaxis.”
Do you treat anaphylaxis with sugammadex? The jury’s out. No one’s officially said yes or no. There’s case reports that suggest that it works really well. I would argue that if you’ve got an anaphylactogenic drug floating around in your plasma, it’s going to keep triggering any mast cells that weren’t triggered or are partially triggered until your liver clears it. Mopping that up probably is only a good thing. And I would, nine times out of ten, I think, give it, and I have given it for rocuronium anaphylaxis in the single event.
Pharmacological Principles: Bowman Principle
08:14-08:47
Rocuronium is less potent than vecuronium. I mentioned vecuronium earlier. This is to illustrate a principle called Bowman principle. Bowman principle suggests that if you are using a less potent agent, you have to give more of it in order to have the same effect. However, because you’re adding more and it’s a competitive molecule, you actually paradoxically achieve a faster onset time than you would otherwise expect with a supposedly weaker drug.
The other thing to note with vecuronium as another aminosteroid is sugammadex works for vecuronium too.
Examination Context and Future Topics
08:47-10:28
In summary, rocuronium is a really commonly used drug that you certainly need to be familiar with, and you’re going to get examined on, at least in part, about the agent itself, before the examiner then wants to explore such concepts as the neuromuscular junction, the interplay between acetylcholine, rocuronium and reversal approaches, or how to go about understanding the depth of paralysis your patient is currently experiencing.
We’re talking train of four monitoring being that objective or subjective monitoring. They may ask about objective approaches to measuring the train of four, be that accelerometers or electromyography of the muscle itself, to understand how deeply anaesthetised your patient is and/or how reversible they are, as well as the sequelae of incomplete reversal in patients, which you could accidentally have a paralysed patient in recovery and you’re going to feel very sheepish when that happens if you’ve not done it properly and thought hard about it.
Always be reversing. Some of the bosses might not bother. Always be reversing, unless there’s a contraindication to the…
Future podcasts. We’re going to talk in great detail about acetylcholine. We’re going to talk about how you trigger that saltatory conduction down your nerve sheath to get to your neuromuscular junction in the first place, going to explore the delights of how excitation-contraction coupling comes about, what other drugs, agents, and toxins can influence your muscle power and whereby they act, and naturally we’re going to talk about suxamethonium, atracurium, sugammadex, neostigmine, and glycopyrrolate. But we’re getting carried away.
Conclusion and Call to Action
10:28-10:59
See you next time. If you found it useful or awful, please like and subscribe and rate the show. Definitely check out the show notes for those diagrams and the detail of this content. It is a bucket of content to get to grips with. Keep working at it, and you will get better, faster, and stronger. It is vital to keep your interest alive for the science that we’re covering and not overcook yourself. You will be amazed by what you know come exam day. Don’t freak out, keep studying.
Enjoyed this? Review on Apple Podcasts Rate on Spotify
Support the show Help keep the lights on SBA question bank @ Teach Me Anaesthetics