Sugammadex For Anaesthetists
1 April 2026
Contents
Introduction
Sugammadex changed the game for neuromuscular blockade reversal. Before it came along, your only option for reversing a non-depolarising block was neostigmine, which meant waiting until the block was shallow enough, co-administering glycopyrrolate or atropine to manage the cholinergic side effects, and accepting that residual paralysis was still a possibility in recovery. Sugammadex sidesteps all of that. It is a modified gamma-cyclodextrin that directly encapsulates aminosteroid neuromuscular blocking agents, principally rocuronium and to a lesser extent vecuronium, forming a tight 1:1 complex that is biologically inert and renally excreted unchanged.
It is like a UFO abducting all the rocuronium.
You can now reverse a patient from profound rocuronium-induced paralysis within minutes, at any depth of block, without needing to worry about side effects or ensuring a minimum number of twitches on the nerve stimulator first. It has also made rocuronium RSIs considerably less anxiety-inducing, because you have the option of a 16 mg/kg rescue dose if things go sideways at induction.
In this episode we cover the pharmacology of sugammadex from the ground up: its physico-chemical properties, mechanism of action, dosing by depth of block, pharmacokinetics, side effect profile, and the clinically relevant interactions you need to know about, including the contraceptive interaction and fabulous flucloxacillin philandering with the encapsulated rocuronium question. We also look at the evidence around sugammadex-associated anaphylaxis and talk through the practicalities of rescue reversal in a difficult airway scenario.
Sugammadex Pharmacology
Sugammadex is a modified gamma-cyclodextrin with a hydrophobic interior cavity that selectively encapsulates the steroidal ring structure of aminosteroid neuromuscular blocking drugs, forming a biologically inert water-soluble complex excreted renally unchanged.
Sugammadex Physico-Chemical Properties
| Name | Sugammadex Su=sugar, gammadex= gamma cycloDextrin Brandname Bridion®! |
| Class | Modified gamma cyclodextrin / Selective relaxant binding agent (SBRA) |
| Chemical Make Up | Gamma cyclodextrins were studied and utilised in the food industry and to deliver drugs that were otherwise not very soluble in water. |
| History | First approved for use in the EU in 2008, with FDa approval in 2015 |
| Colour/Appearance | As a clear colourless, solution for injection. 100mg/ml 200mg and 400mg ampoules Store below 30 °C pH 7-8 300-500mOsm/kg One ml contains 9.7mg NaCl |
| Molecular weight | 2178 g/mol (Hefty!) |
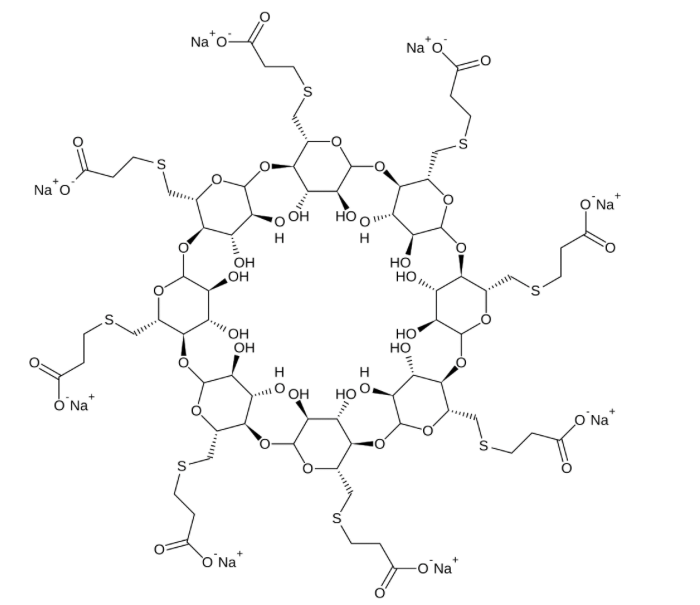
{kind=link}
3D structure resembles a truncated cone or donut
Hydrophobic (lipophilic) cavity and a hydrophilic exterior.
Rocuronium has four hydrophobic steroidal rings
As Frank managed to make it to a published post, he deserves to stay, but he has been supplanted by an actual Sugammadex molecule.

Sugammadex Pharmacodynamics and Side Effects
| Mechanism of Action | Acts by Encapsulating the steroid portion of the aminosteroid relaxant molecule within its Hydrophobic interior Water soluble complexes, at a 1:1 ratio The negatively charged carboxyl groups bind to the positively charged nitrogen atom on the aminosteroidal molecule. + van der waal forces and possibly some witchcraft. Binds tightly, with negligible rates of dissociation. This binding of the neuromuscular blocking drug – leads to a decrease in free circulating drug > change in concentration gradient > depletion of agent at NMJ > facilitation of ACh action in the NMJ. Biologically inactive in itself. |
| Chief Effect / Actions | Near magical reversal of rocuronium paralysis. |
| Dose | IV Single bolus -Works quicker with rocuronium than vecuronium, also encapsulates pancuronium (but not very well) 4mg/kg if 1-2 post tetanic counts present. 2mg/kg recommended when T2 NMJ block (fade is present) Rescue Reversal = 16mg/kg. (if given 3 mins post 1.2mg.kg RSI dose takes 1.5 mins to reverse) If block re-establishes then further 4mg/kg 1.2mg rocuronium/kg then after 3 mins 16mg sugammadex/kg will reverse a patient faster than waiting for 1mg/kg of suxamethonium to resolve. Humans were given 0.6mg/kg rocuronium, and then 3 mins later given 8mg/kg sugammadex, leading to tof >0.9 in 2 minutes. if 4mg/kg was given, it took <4 mins for same recovery. |
| Side Effects | Headline : Sugammadex is highly inoffensive and causes no apparent mischief (bar Anaphylaxis, and impaired COCP function) |
| Cautions | Can’t use rocuronium to reliable effect for ~24 hours, And if immediately reaching for an agent to re-paralyse with when the patient gets Sugammadex anaphylaxis, you may well find that its onset is rapid, if there is remnant rocuronium still lurking at sub therapeutic amounts. Remember that the neuromuscular junction will work with 70% of N2s still occupied. thus when you give the Atracurium in a desperate rescue it doesn’t have as much work to do. |
Sugammadex Pharmacokinetics
| Absorption | n/a |
| Distribution | Volume of distribution 11-14 L No plasma protein binding |
| Metabolism | Nil |
| Elimination | Half-life 1.8 Hours 88-120ml/min Clearance Renally cleared complex. |
Sugammadex in Anaesthesia
Sugammadex interacts with several co-administered drugs because its hydrophobic cavity is not entirely selective for aminosteroid NMBDs; the clinically significant interactions are the combined oral contraceptive, flucloxacillin, and fusidic acid.
What else could sugammadex bind ?
its 120x less enamoured with aldosterone/cortisone/hydrocortisone, and even less interested in (400-700x less) atropine/verapamil, phentolamine, naloxone and ketamine.
But it is known to quite fancy a spot of circulating synthetic sex hormone – as the steroid in aminosteroid is indeed a synthetic sex hormone. And Sugammadex on the same day as a OCP needs to be treated like a missed pill day as it binds to the progesterone element, (barrier precautions for 7 days)
Interestingly Flucloxacillin and fusidic acid (both Antibiotics) can trigger a displacement of rocuronium from sugammadex, so you theoretically ‘reverse the reversal’ somewhat with a dose of emergency flucloxacillin. Suxamethonium or Atracurium is likely a better choice…..
Remember, the same amount of rocuronium is inside your patient pre and post sugammadex, it is just not able to get at the nicotinic acetylecholine receptors in the NMJ, so if it were to some how get displaced, you would return to your prior state of neuromuscular blockade.
Contraceptives
As Sugammadex takes a fancy to circulating steroids, oral contraceptives are in the firing line here and their efficacy may be impaired for a number of days
Sugammadex anaphylaxis
Yes, Sugammadex can cause anaphylaxis.
Yes you will be very unfortuante to have a patient, reversed from their neuromuscular blockade, and possibly even extubated before you noticed the development of this life threatening IgE mediated distributive shock.
Even worse, they have been wheeled around to recovery, they look a little sleepy and then you figure it out in the middle of PACU!
Evidence and incidence – 2024 retrospective Australian multicentre analysis at 6 allergy centres.
Suggested incidence is 1:23934 sugammadex administrations
Higher incidence reported in Japan, 1:2500 ( to 1:20K)
suggestions that the incidence may increase overtime as more patients are exposed and then re-exposed to sugammadex, its worth noting that cyclodextrins are found as food preservatives, as drug carriers and in other products.
Savic et al note that the Japanese 1:2,500 figure was based on clinical suspicion rather than confirmed tryptase rise or allergy clinic diagnosis. Teicoplanin is the most anaphylactogenic drug we use routinely rocking at at 1:6500 incidence.
Rescue reversal
If you’re in a situation where this may be needed, have the ampoules out, know how many you intend to put in the patient, and ensure whoever is drawing it up probably draws one up and gives it and then draws up the next, as drawing up 5 amps and then injecting might lead to a longer duration of non-return of muscle power.
This does assume that the patient wants to breathe….. if you also narcotised them with remifenatnil or a very healthy dose of something else. then they will need naloxone too
This does assume that the dose of hypnotic agent has not been so sufficient as to obtund the patients interest in breathing also. (less of an issue as the kinetics of propofol lead to transient apnoeas at best, unless you’ve given a larger than normal dose to try and gain control of a challenging to ventilate patient type of situation.
Summary
Sugammadex (Bridion) is a modified gamma-cyclodextrin and selective relaxant binding agent. It works by encapsulating the steroidal ring structure of aminosteroid neuromuscular blocking drugs within its hydrophobic cavity, forming a water-soluble 1:1 complex held together by electrostatic forces, van der Waals interactions, and possibly magic.. The bound rocuronium is rendered biologically inactive, creating a concentration gradient that draws free drug away from the neuromuscular junction.
Key points for the FRCA Primary:
- Class: modified gamma-cyclodextrin (selective relaxant binding agent)
- Mechanism: direct encapsulation of aminosteroid NMBDs (rocuronium >> vecuronium > scant pancuronium)
- Dosing: 2 mg/kg at reappearance of T2; 4 mg/kg at 1-2 post-tetanic counts; 16 mg/kg for rescue reversal
- Pharmacokinetics: Vd approximately 11-14 L (roughly ECF volume), no protein binding, no hepatic metabolism, renally excreted as the sugammadex-rocuronium complex, half-life approximately 1.8 hours
- Side effects: remarkably few at therapeutic doses. Anaphylaxis is the headline concern, with reported incidence around 1:24,000 administrations (higher figures reported from Japan, though these may reflect clinical suspicion rather than confirmed allergy clinic diagnoses)
- Contraceptive interaction: sugammadex binds circulating progesterone, so administration on the same day as a combined oral contraceptive should be managed as a missed pill
- Re-paralysis: rocuronium will not be reliably effective for approximately 24 hours post-sugammadex. If you need to re-paralyse urgently, reach for suxamethonium or a benzylisoquinolinium agent such as atracurium
- Flucloxacillin and fusidic acid can displace rocuronium from sugammadex in vitro, though the clinical significance of this remains unclear [fabulous flucloxacillin philandering].
- The same total amount of rocuronium remains in the patient after sugammadex administration. It has not been eliminated, it has been encapsulated. If displacement were to occur, the block would return.
Sugammadex to reverse rocuronium anaphylaxis?
It might work, and now I know its odds of causing anaphylaxis itself are lower than I thought, I might be tempted.
There are lots of case reports suggesting it helps, and some suggesting it does not.
I have been in a situation where we gave some for a presumed roc anaphylaxis – and it did not help (it could be anaphylaxis to many other things too tho) We gave it late, when the cascade of histaminey serotonin madness was in full swing.
References
- Crimmins D, Crilly H, van Nieuwenhuysen C. Sugammadex hypersensitivity: a multicentre retrospective analysis of a large Australian cohort British Journal of Anaesthesia, 2024; 134, 72-79
- Chia, Pamela A. MD, MS; Wolfe, Michael W. MD. Sugammadex-Associated Anaphylaxis: Summary and Proposed Management. Anesthesia & Analgesia 139(2):p 273-277, August 2024. | DOI: 10.1213/ANE.0000000000006759
- Managing the risk of contraceptive failure with sugammadex. RCoA Bulletin Spring 2024.
- Savic LC, Kaura V, Muthukumar N, Hopkins PM. Sugammadex-associated anaphylaxis: time to act. Br J Anaesth. 2023;130(5):553–556.
Common questions
What is sugammadex and how does it work?
Sugammadex (brand name Bridion) is a modified gamma-cyclodextrin classified as a selective relaxant binding agent (SRBA). It works by encapsulating the steroidal ring structure of aminosteroid neuromuscular blocking agents, principally rocuronium, within its hydrophobic cavity. This forms a water-soluble 1:1 complex held together by electrostatic forces and van der Waals interactions, with negligible dissociation. By scavenging free rocuronium from plasma, sugammadex creates a concentration gradient that draws the drug away from nicotinic acetylcholine receptors at the neuromuscular junction, producing rapid reversal of paralysis.
What are the dosing guidelines for sugammadex by depth of neuromuscular blockade?
Sugammadex dosing is guided by train-of-four (TOF) monitoring: 2 mg/kg at reappearance of the second twitch (T2) — i.e. at least two twitches of the train-of-four; 4 mg/kg when the block is deep with 1–2 post-tetanic counts but no TOF response; and 16 mg/kg for rescue reversal in a cannot-intubate-cannot-oxygenate scenario. At the rescue dose, given 3 minutes after a 1.2 mg/kg RSI dose of rocuronium, full reversal occurs in approximately 1.5 minutes.
What are the key pharmacokinetic properties of sugammadex?
Sugammadex has a volume of distribution of 11–14 litres (approximately extracellular fluid volume), no plasma protein binding, and undergoes no hepatic metabolism. It is renally excreted unchanged as the water-soluble sugammadex–rocuronium complex, with a half-life of approximately 1.8 hours and clearance of 88–120 mL/min. In patients with severe renal impairment, the complex cannot be excreted effectively, which should inform the choice of neuromuscular blocking agent.
Can you re-paralyse a patient with rocuronium after giving sugammadex?
No. Rocuronium cannot be reliably re-administered for approximately 24 hours after sugammadex, as the drug remains encapsulated in the sugammadex complex within the body. If urgent re-paralysis is required, an alternative agent should be used: either suxamethonium (a depolarising agent) or atracurium (a benzylisoquinolinium non-depolarising agent). Because sugammadex only reduces rocuronium receptor occupancy to around 40%, a dose of atracurium may achieve effective paralysis more quickly than expected.
What is the risk of anaphylaxis with sugammadex?
Sugammadex can cause IgE-mediated anaphylaxis. Early Japanese data suggested an incidence as high as 1 in 2,500, but a more robust 2024 Australian multi-centre retrospective analysis using confirmed allergy centre diagnoses found an incidence of approximately 1 in 23,934 administrations. The risk may increase with repeated exposure, and background sensitisation to cyclodextrins found in food preservatives and other pharmaceutical products is a theoretical concern. For context, teicoplanin carries a higher anaphylaxis risk at approximately 1 in 6,500.
Does sugammadex interact with oral contraceptives?
Yes. Because the aminosteroid backbone of rocuronium is a synthetic progesterone analogue, sugammadex also has affinity for circulating synthetic sex hormones found in combined oral contraceptive pills and progesterone-only pills. Administration of sugammadex on the same day should be treated as a missed pill, and barrier contraceptive precautions are recommended for seven days following administration.
Thanks for listening. Take it day by day, don't overcook yourself — keep studying.
Transcript
38 min listenRead the full transcript
Gas Gas Gas – EduCast: Sugammadex
Cleaned and Consolidated Transcript
Host: James | gasgasgas.uk
Introduction
00:00–01:15
- Final episode in the neuromuscular blocking agent series, covering sugammadex.
- Gas Gas Gas has surpassed 100,000 listens since inception.
- Sugammadex was historically very expensive but is now approximately £3.40 per box of ten 200 mg vials.
- Clinicians are increasingly reaching for sugammadex over glycopyrrolate–neostigmine.
Hello, Team Anaesthesia. Welcome to Gas Gas Gas. This is the best anaesthetic science podcast for the FRCA Primary exam. Our goal is to fill your brain with all this highly useful information. Now you might be in the gym right now, commuting, or ironing your scrubs, and there’s no judgement here. Gas Gas Gas will prime your brain for the monsoon of knowledge you need to imbibe. The revision is eventually going to end, but for now, expect facts, concepts, model answers, and the odd tangent. Now remember to check out the website, that’s gasgasgas.uk. There are show notes there, with all the detail, plus links to foundational reference papers and anything else useful I find for you guys. Anyway, buckle up, get ready for your mind to be bent into a new shape, and let’s get on with the show.
Hello everyone, welcome to the Good Friday episode of Gas Gas Gas. I’ve been released from the intense rigours of baby-caring duty for the next forty-five minutes or so, which is a delight. I hope you have some decent plans for your Easter Sunday and perhaps the following week you can catch up on all that paperwork that hasn’t been happening.
Why Sugammadex Matters
01:15–03:00
- Sugammadex is now cheap and is used far more frequently than glycopyrrolate–neostigmine.
- It closes the neuromuscular blocking agent series as the most significant modern development in anaesthetic pharmacology.
Today we’re talking about sugammadex. Now, when I was very much starting out, and even when I was a wee foundation doctor trying to venture forth into theatres to try and see what all this confusing stuff is about with drugs and knocking people unconscious, there was always, “Oh yes, and you could reverse this drug with sugammadex, but you have to sign it out from the cupboard and trade an arm for it.” So we weren’t generally allowed to use it.
And that was when sugammadex was really, really expensive. Nowadays it’s £3.40 in my trust for a box of ten 200 milligram vials of sugammadex and it’s being used liberally. Folks are definitely reaching for it more than glycopyrrolate–neostigmine. And so it seems fitting to close out our paralysing agent episodes with the one new, cool, interesting, and modern thing that’s really happened in anaesthetic pharmacology for quite some time.
Limitations of Pre-Sugammadex Reversal
03:00–05:00
- Previously, the only option for reversing non-depolarising muscle relaxants was acetylcholinesterase inhibitors (neostigmine, pyridostigmine).
- Neostigmine cannot overwhelm profound competitive blockade from rocuronium at high receptor occupancy.
- Neostigmine’s muscarinic side effects require co-administration of anticholinergics (e.g. glycopyrrolate), adding further side effects: PONV, tachycardia.
- Rocuronium RSI in a difficult airway was a bold choice when you couldn’t reliably undo the paralysis.
- Suxamethonium provides only approximately 1.5–2 minutes of optimal intubating conditions, with diminishing conditions on repeated attempts.
Sugammadex certainly did change the game for neuromuscular blockade. Previously your only option for reversing a non-depolarising muscle relaxant was acetylcholinesterase inhibitors, and neostigmine and sometimes pyridostigmine were the ones that were picked. But it had some faults in that you couldn’t just give someone rocuronium and then chuck some neostigmine at them and it would all get better, because it simply doesn’t have the capacity to overwhelm the competitive nature of rocuronium at those concentrations of acetylcholine that it can muster.
And naturally neostigmine has side effects which have to be countered by anticholinergics, and anticholinergics have side effects themselves. So patients might feel a bit grottier, more post-op nausea and vomiting, maybe a tachycardia. It’s not perfect, but it did the job when we wanted to get people over the hill when they’re almost fully returned to muscle strength. You would nudge them over with neostigmine.
Which meant that it was quite bold to do a rocuronium RSI in someone with a difficult airway when you couldn’t undo that problem. And that’s where suxamethonium generally found its position. The other thing to note was suxamethonium wasn’t without its problems. You know, it’s got a honking side-effect profile that you definitely should be able to barf out in an exam. And if you can’t intubate: A, it’s quite a long time before it wears off really, and B, the more you muck around with the airway and try again and again, the less effective your intubating conditions become. And then you might end up in a situation where they’re not quite paralysed, but a little bit paralysed, might be thinking about trying to have some laryngospasm, and you’ve got this difficult airway and it all becomes a bit of a torrential disaster.
Sugammadex Enters the Scene
05:00–06:11
- Sugammadex enables rapid reversal of profound rocuronium paralysis.
- Transforms the RSI paradigm: rocuronium can be given with confidence, and if intubation fails, neuromuscular blockade can be reversed.
But then sugammadex rolled up its sleeves and came into the ring. It sidesteps all these problems. It brought us into a world where you could reverse profound rocuronium paralysis really spectacularly fast with one whacking dose of a drug, turning those considerably anxiety-inducing situations of “Well, we’ve got to use sux because it needs to wear off, but we probably only have a minute and a half to two minutes of actual decent paralysis, so we’d best get it right” into: rocuronium, whereby you wait a minute, you’ve had a look-see, didn’t go quite to plan, let’s just have a rethink. And their neuromuscular blockade over that time has gotten deeper, acceptably so. And if you decide to bail out because you can’t quite achieve what you want to achieve – boom, reversed.
So this episode will cover the pharmacology of sugammadex: its physicochemical properties, mechanism of action, how you might go about dosing it, the kinetics, the side-effect profile, and some little interesting foibles that have progressively come to light with it.
Physicochemical Properties
08:06–10:00
- Name derivation: Su (sugar) + gamadex (gamma cyclodextrin).
- Brand name: Bridion (UK).
- Modified gamma cyclodextrin with eight additional side chains enhancing affinity for rocuronium.
- Cyclodextrins are used in industry for drug delivery (delivering water-insoluble substances to aqueous environments).
- First EU approval: 2008; US FDA approval: 2015.
- Presentation: clear, colourless solution for injection, 100 mg/mL; available in 200 mg and 400 mg ampoules.
- Storage: below 30°C. pH: 7.8.
- Osmolality: 300–500 mOsm/kg (slightly hyperosmolar).
- Molecular weight: 2,178 g/mol.
So, sugammadex: ‘Su’ means sugar in the name, ‘gamadex’ is gamma cyclodextrin. Its brand name is Bridion in the UK. It’s a modified gamma cyclodextrin. Cyclodextrins are found in a number of places in industry, in food preservation and drug delivery. But they modified it and added eight extra arms that change the shape slightly and make it quite a bit more fanciful for rocuronium.
The reason it’s used in industry in drug delivery is because things that aren’t very soluble in water can be delivered to watery places using a gamma cyclodextrin as a vector. And some clever boffin thought, “Oh, what if we did this the other way round and mopped up something with it?”
First approved for use in the EU in 2008. US FDA approval in 2015. So we’re ahead of the curve. It is a clear, colourless solution for injection, coming in 100 milligrams per mL, and generally you get it in 200 mg ampoules and 400 mg ampoules. I always do seem to remember that it always used to be in the cupboards at 400 when it was expensive, as if the manufacturers were being a bit sneaky. You have to store it below 30°C. It has a pH of 7.8. It’s a little bit hyperosmolar compared to blood, 300 to 500 milliosmoles per kilo. And it is a chonking molecule, as you might expect, at 2,178 grams per mole. Hefty.
Molecular Structure and Mechanism of Action
10:00–13:30
- 3D structure: truncated cone / stretched doughnut with a hydrophobic (lipophilic) cavity and hydrophilic exterior.
- Rocuronium and vecuronium have four hydrophobic steroidal rings (aminosteroid backbone = synthetic sex hormone analogue).
- Sugammadex encapsulates the steroid portion, forming a water-soluble 1:1 complex.
- Binding: negatively charged carboxyl groups bind positively charged nitrogen atoms on the aminosteroid; van der Waals forces also contribute.
- Negligible dissociation once bound.
- Mechanism: sugammadex scavenges free plasma rocuronium → creates steep concentration gradient → rocuronium moves out of NMJ into plasma → rapid offset of paralysis.
Now, check out the sugammadex molecule. You can either go on the show notes to do that, or you can just Google sugammadex. And it’s quite pretty in its carbon skeleton layout. In 3D form, it resembles a truncated cone or like a slightly stretched-out doughnut, where it’s got a dominant ring area, and then a slightly funnel-like bit that extends the space within which rocuronium can be tempted forth.
The cavity is hydrophobic, i.e. lipophilic. And the exterior is hydrophilic. So the exterior bit loves to be in contact with water, the interior bit less so. And rocuronium, alongside vecuronium, has four hydrophobic steroidal rings. Remember: aminosteroid – the steroid backbone of these drugs is a synthetic sex hormone. That’s what they plonk the acetylcholine-mimicking moieties onto to develop these non-depolarising muscle relaxants.
So sugammadex’s mechanism is to encapsulate the steroid portion of the aminosteroid part of the molecule, forming a water-soluble complex – because it would be a bit daft if rocuronium bound to it and then it became less soluble in the plasma. Presumably that would be hard work for the body to tidy up and require more metabolism. And it complexes at a one-to-one ratio, so one sugammadex binds to one rocuronium.
The negatively charged carboxyl groups bind to the positively charged nitrogen atoms on the aminosteroid. There are also some van der Waals bonding forces happening. So it thus binds tightly to rocuronium with negligible rates of dissociation. Once that rocuronium is snaffled up by the sugammadex, it is quite unlikely to dissociate.
How this leads to a reversal of paralysis is because you’ve altered the concentration gradient. Remember, rocuronium is normally dancing into that neuromuscular junction, messing with the nicotinic receptor, but then it might dissociate from that nicotinic receptor, float off for a bit, but then another rocuronium comes in, and because there’s a greater quantity of rocuronium around than acetylcholine, it outcompetes the acetylcholine and keeps you paralysed.
You end up with a neat and tidy equilibrium of rocuronium at the neuromuscular junction versus rocuronium in plasma, but naturally your liver is mopping up rocuronium slowly from the plasma normally, and you get a diminishing quantity of rocuronium at the neuromuscular junction over time. Sugammadex replaces the role of that slower liver metabolism by basically chomping it up, markedly increasing the gradient of rocuronium in plasma versus rocuronium at the neuromuscular junction. It likes a nice equilibrium. More rocuronium moves out into the plasma to keep it even and tidy. But there’s sugammadex waiting in the dark corridors of your capillaries. And it continues to tidy it up as long as there is sugammadex available. And that’s why you see such a rapid offset.
It’s kind of like the reverse of an RSI dose of rocuronium where you’ve filled that plasma with rocuronium and it all piles forth into the neuromuscular junction. So like a big Ctrl+Z, Cmd+Z undo button. And that’s why its chief mechanism of action is near-magical reversal of rocuronium paralysis. And the first time I gave it, I was just like, “Wow, that’s amazing. They were floppy and now they’re not.”
And if you were to be asked a question about what would be a near-ideal drug in anaesthesia, the answer could be propofol, because it’s very convenient, but actually sugammadex is now probably the interesting winner in that question, because it achieves all those things beautifully.
Side-Effect Profile
13:47–15:27
- Almost biologically inactive – minimal side effects.
- Anaphylaxis: initial concern from Japanese data (~1 in 2,500), now estimated closer to 1 in 20,000–25,000.
- Oral contraceptive interaction: sugammadex binds the steroidal component of aminosteroids (synthetic progesterone analogues), impairing COCP and POP function.
- Barrier precautions for seven days recommended post-administration.
And what is its side-effect profile? Barely anything. It is almost biologically inactive. And that’s just great, isn’t it?
What can it do to people? So it does cause anaphylaxis. And there was a bit of a higher concern about the potential for sugammadex to cause anaphylaxis around the time when it was starting to come off patent. In Japan they had noted that it seemed to cause quite a high frequency of anaphylaxis, one in two and a half thousand, based on some research they’d done there. It was subsequently picked up in Australia with a study that was perhaps a bit more robust, that suggested no, it probably wasn’t one in two and a half thousand, but perhaps more near one in twenty-five thousand. So it can cause anaphylaxis.
The other problem is that it can fiddle around with the combined oral contraceptive pill and the progesterone-only pill. Remember, rocuronium, vecuronium, and pancuronium are aminosteroids. The steroid backbone is a synthetic analogue of progesterone, which sugammadex binds to. Therefore it impairs the function of these oral contraceptives. And you do not want a patient saying, “I got pregnant because you gave me sugammadex.” Tell the patient. Barrier precautions for seven days.
Dosing
15:27–20:00
Rescue Reversal (Can’t Intubate, Can’t Oxygenate)
- 16 mg/kg.
- At 3 minutes post-RSI dose (1.2 mg/kg rocuronium), full reversal in approximately 1.5 minutes.
- Pre-calculate and draw up the dose if you anticipate difficulty (e.g. 75 kg patient = six 200 mg ampoules = 1,200 mg).
- Reversing paralysis does not reverse respiratory drive depression from other induction agents – consider naloxone, residual propofol effect on airway tone.
Moderate Block (Fade Visible on Train-of-Four)
- 2 mg/kg.
- Appropriate when four twitches present but with visible fade.
- Allow approximately 5 minutes for maximal effect.
Deep Block (No TOF, PTC ≥1–2)
- 4 mg/kg.
- Use post-tetanic count when no train-of-four twitches visible.
- Keep nerve stimulator attached and recheck after a few minutes.
- Remember: the nerve stimulator hurts when the patient is awake – don’t stimulate at a MAC of 0.2.
The dosing. How do you dose sugammadex? You need to use train-of-four, unless you are bailing out of dodge, you’ve given your large dose of rocuronium, and it’s all gone pear-shaped. In which case you give 16 milligrams per kilo. And say you’ve given your 1.2 milligram per kilo dose of rocuronium, you’ve mucked around for three whole minutes trying to get a tube in and thinking, “This is going very wrong.” The patient’s now very blue. At three minutes, if you give 16 milligrams per kilo of sugammadex, it will take 1.5 minutes to fully reverse that patient.
Now just because you’ve fully reversed their paralysis doesn’t mean you’ve fully reversed their interest in breathing. Although you would presume if they were blue, they probably do have quite a high CO₂. There’s a degree of motivation there. But it’s not a perfect drug here. You might think, “Oh, well, give some naloxone as well.” Definitely give them a drive to breathe. You still may have some loss of airway tone with your dose of propofol. So it’s not an “it’ll all make it better” drug, but with common sense and thought you can probably undo most of what you’ve done to try and retrieve the situation at hand.
I always think that if you are definitely in a precarious situation, and it’s on your mind that you may wish to reverse them, pre-calculate your dose, because 16 milligrams per kilo is quite a lot of sugammadex. If you had a 75 kilo patient, you are drawing up six ampoules of 200 milligram sugammadex. You should just have them on the side as a pre-calculated rescue dose.
Now if we’re back to the end of the case, patient’s a bit paralysed, how much should I give? You have two choices here: 2 mg or 4 mg per kilo. Although in reality, 200 mg of sugammadex or 400 mg of sugammadex. If you can see fade on your train-of-four – so you’ve got four twitches and the first one is quite reasonable amplitude, but then it diminishes off and you can barely see the fourth one – then 2 milligrams per kilo will work. And remember you see effect quite quickly, but it doesn’t just immediately stop working, because we all know that kinetics of drugs are not linear. There are diminishing returns over time as you suck out smaller and smaller fractions of rocuronium from the neuromuscular junction. So, in an ideal world, someone who’s fairly paralysed, you should give the sugammadex like five minutes to work, probably. And that would be more than enough to see the maximal effect of that dose.
If you are in a situation where you’ve not got enough twitches, do not fear. Do a post-tetanic count. Because remember we can’t move our arms and legs unless we’ve got 5% of our nicotinic receptors available, in which case you see a twitch. You’ll see three to four twitches if you have between 25 and 35% of your receptors available. So we’re just trying to really get patients down to having perhaps 40% of their receptors available to acetylcholine, and then you will see depolarisation and muscle control.
Even the deepest, darkest “Oops, I gave some rocuronium and then they started closing – oh, what have I done?” moments can be recovered. But you should use the post-tetanic count to understand the level of paralysis in this deep plane of neuromuscular blockade. And that’s where you do a tetanic stimulus and then a zap every second and you count how many you see. And if you see more than two, then you can use 4 milligrams per kilo of sugammadex and make it all better.
Now, if you are in this situation and you’ve done a bit of a whipsy-daisy and given a bit more paralysis than the boss might have done, it would be sensible to give the sugammadex with the nerve stimulator still on, give it a few minutes, and then check their twitches again and be sure that you have achieved adequate reversal in that situation. And remember, the nerve stimulator hurts when you’re awake. So don’t be twitching a patient who’s got a MAC of 0.2. You might wake them up, and that’s probably not the nicest thing you could do.
Post-Reversal Limitations
19:54–22:44
Cannot Re-use Rocuronium
- Rocuronium cannot be reliably re-administered for 24 hours after sugammadex.
- If re-paralysis is needed, use atracurium or suxamethonium.
Receptor Occupancy and Re-paralysis with Atracurium
- Only ~60% rocuronium receptor occupancy (40% available to acetylcholine) is needed for adequate muscle power.
- Atracurium goes quite a long way post-reversal – potentially achieving RSI-like conditions.
- Niche consideration: in cases where extubation problems are anticipated, titrating sugammadex carefully may make it easier to regain control.
So what’s the other problem with sugammadex reversal? Well, you can’t use rocuronium again, can you? Not reliably for 24 hours. So if you find yourself in a spot of bother where you’ve pulled the tube and then your patient’s going and turning blue and it’s all going horribly wrong for some unexpected reason, you can’t give rocuronium to fix the problem. So you would need to dose them with atracurium or suxamethonium, both of which will work.
[Teach Me Anaesthetics sponsor segment – 20:25 to 21:47]
Now interestingly, I’ve reminded you guys that we only need to get receptor occupancy down to like 60% rocuronium, 40% available to acetylcholine, to see good muscle power. That means that your dose of atracurium actually goes quite a long way. You may even get them looking like they’ve had an RSI with atracurium because you’ve not got to go as far as that dose of atracurium you might have given at the start to achieve overwhelming receptor occupancy once again. And that’s a bit of a gift, if it all were to go unexpectedly tricksy.
There could be an argument there for niche cases to be very careful in the amount of sugammadex you give, instead of just being a bit lackadaisical and saying, “Oh, just give them 400, whatever,” if you were to expect extubation problems, because then it’ll be easier to regain control of the situation. Just a thought. That’s very niche, and you probably don’t need to think in that much detail.
Pharmacokinetics
22:48–24:48
- Absorption: IV only (no clinically useful oral bioavailability).
- Volume of distribution: 11–14 litres.
- Plasma protein binding: none.
- Metabolism: none.
- Elimination: renally cleared (as water-soluble complex).
- Half-life: 1.8 hours.
- Clearance: 88–120 mL/min.
- Clinical implication: in patients with severely impaired renal function, the sugammadex–rocuronium complex is not excreted. Consider whether atracurium would have been a more sensible choice.
Kinetics of sugammadex. Absorption – well, I couldn’t find anything that would suggest that when you eat it, you absorb it. It has been used as a food preservative. So it’s probably safe to eat. Cyclodextrins have various uses. Where else do you find cyclodextrins? Well, there’s a variant of cyclodextrin in Febreze. That does that clever thing they say where it sucks up the smell molecules and makes it all better. Does it irreversibly bind the smell molecules? Does that just mean the smell molecules are still there but you can’t smell them? And if that breaks down, the smell comes back. Who knows? This isn’t an episode about Febreze.
The volume of distribution of sugammadex is 11 to 14 litres, and there’s no plasma protein binding involved. Do you metabolise it? No, you hecking don’t. Cracking. How do you get rid of it? It’s renally cleared. So if you’ve given sugammadex to someone who you’ve given rocuronium to who just so happens to have absolutely crocked kidneys, you probably can’t give rocuronium to them for a really, really, really long time because they’re just not going to pee it out. And in that situation, you just maybe need to think whether or not that is the best method of reversing the patient and whether or not atracurium might have been a more sensible choice.
Half-life is 1.8 hours. Clearance is 88 to 120 mL per minute. That’s quite an easy drug to learn and remember because you can reliably say that there’s no metabolism, it’s renally cleared because it’s water-soluble, 11 to 14 litre volume of distribution, doesn’t bind to proteins. Cracking. Very minimal side-effect profile, causes anaphylaxis, careful with your oral contraceptives. They could ask you a bit more about the science behind it. It is probably going to be a very, very commonly used drug from now on. So they could rightly justify saying, “Well, if you’re using it every day, you should understand it.”
What Else Can Sugammadex Bind?
24:48–26:44
Relative Binding Affinities
- Aldosterone, cortisone, hydrocortisone: 120× less affinity than rocuronium (slight binding).
- Atropine, verapamil, phentolamine, naloxone, ketamine: 400–700× less affinity (negligible clinical significance).
- Verapamil: non-dihydropyridine calcium channel blocker (“Verapakill” if given alongside beta-blockers).
- Phentolamine: alpha-blocker, used in phaeochromocytoma surgery.
Oral Contraceptive Interaction
- Sugammadex binds circulating synthetic sex hormones (aminosteroid backbone is a synthetic progesterone analogue).
- Renders COCP and POP non-functional – treat as a missed pill day.
- Barrier precautions for seven days recommended.
Now for a bit of interest. What else could sugammadex bind to? Studies have shown that if you make a comparison between sugammadex’s interest in rocuronium and compare it to other things: aldosterone, cortisone, and hydrocortisone are 120 times less interested in sugammadex than rocuronium. But they do bind a little bit. And then interestingly, 400 to 700 times less: atropine, verapamil, phentolamine, naloxone, and ketamine can be bound by sugammadex, but in really quite pathetic fractions that are unlikely to be of any use. Remember verapamil, that’s a non-dihydropyridine calcium channel blocker, sometimes known as “Verapakill,” depending on if you’ve accidentally given it alongside beta-blockers. Phentolamine is an antihypertensive alpha-blocker used in phaeochromocytoma surgery, and we know what naloxone and ketamine are.
What else does sugammadex like? We know that actually it does take quite a fancy to a spot of circulating synthetic sex hormone. As the steroid in aminosteroid is a synthetic progesterone-like hormone. So if you give it to someone who is on the oral contraceptive pill or the progesterone-only pill, you have rendered that non-functional and it needs to be treated like a missed pill day. Now you could argue, well, generally we recommend that people aren’t on the combined oral contraceptive pill if they’re having elective surgery if they’ve got increased risk of VTE, because it increases your risk of clots. But there’ll be a subgroup of people who aren’t at increased risk of VTE who certainly may well be on oral contraceptives. Barrier precautions for seven days are recommended.
Drugs That Displace Rocuronium from Sugammadex
26:49–28:01
- Flucloxacillin and fusidic acid can displace rocuronium from the sugammadex–rocuronium complex.
- Practical advice: if flucloxacillin is requested shortly after sugammadex, wait at least 15 minutes.
- Displacement returns the patient to their prior level of neuromuscular blockade – the same amount of rocuronium is still present.
So there are drugs that can displace rocuronium from sugammadex. I’m sure if you could give these drugs in an inordinately large dose, you could reverse the reversal. And flucloxacillin and fusidic acid, both antibiotics, can trigger this displacement. So I don’t think you’re going to reach for flucloxacillin as an emergency “reverse the reversal” rescue drug. But be wary – if the surgeon’s like, “Oh, you know what, actually, they just need some flucloxacillin,” and you’ve just reversed them with sugammadex, maybe suggest that you should wait a bit. I think the bit of paper I read said wait fifteen minutes. So it’s not really that much to write home about, is it?
And it’s important to bear in mind in this “reverse the reversal” madness that what you have done is taken the rocuronium and prevented it from getting to the neuromuscular junction. The same amount of rocuronium is inside the patient still. So if you were to somehow magically displace it, you would just return to the same amount of neuromuscular blockade that you had previously reversed.
Sugammadex Anaphylaxis
28:01–31:05
- Anaphylaxis: type 1 IgE-mediated reaction → mast cell degranulation → histamine, serotonin, bradykinin, and other vasoactive substances.
- Particular danger: patient has been reversed, extubated, and is in transit when anaphylaxis develops.
- Cannot re-paralyse with rocuronium – must use suxamethonium or atracurium, each with their own risks.
- Japanese data: initially estimated at ~1 in 2,500.
- Australian multi-centre retrospective analysis (2025): 1 in 23,934, confirmed by allergy centre testing.
- Incidence may increase over time with repeated exposures and background sensitisation to cyclodextrins.
So, sugammadex anaphylaxis. If only it didn’t do this, it would certainly be one of the most perfect drugs ever created. So it does do it. Once upon a time we thought, “Oh gosh, it seems to do it quite a bit.” And now we are more of the opinion that it definitely does do it, but it’s not quite so bad.
What is the issue with sugammadex anaphylaxis? Well, one, anaphylaxis is bad for your health. A type 1 IgE-mediated reaction involving degranulation of mast cells where they start hosing out histamine, but also serotonin, bradykinin, and a bunch of other vasoactive substances.
Why are you particularly unfortunate if you’ve given sugammadex? Well, we know that sometimes you get instant anaphylaxis and sometimes it takes a few minutes. You’ve reversed your patient, it’s merrily mopped up the rocuronium, and you’ve extubated them, and now you’re wheeling yourself down the corridor and the sat probe starts going bloop, bloop, bloop, and that lovely waveform disappears and you think, “Oh, the sat probe’s probably fallen off.” Although if you have a trace that wanes as opposed to just disappears, or looks funky, it might be that there’s just no pulsatile flow in their finger anymore.
The patient turns a very funny colour and you’re thinking, “Do I take this one to recovery, or do I reverse back to my lovely anaesthetic room where the drug cupboards are open?” Do you want to be dealing with an anaphylaxis in PACU if you could rather be dealing with it in theatre? Maybe. And obviously you’ve extubated the patient at this point and you can’t paralyse them with rocuronium again. You’ve got to pick a different drug, like suxamethonium or atracurium. One which can cause bronchospasm, malignant hyperthermia, hyperkalaemia, and so on. And the other one which certainly can cause histamine release. Quite the pickle.
So, in Japan, one of their studies noted that the rate of sugammadex anaphylaxis could be as high as one in two and a half thousand. Although further studies have suggested maybe one in 20,000, and a pretty robust 2025 retrospective Australian multi-centre analysis, where data was drawn from allergy centres, noted an incidence of 1 in 23,934 sugammadex anaphylaxis events. And this was allergy centres deciding, “Yes, they do have a reaction to sugammadex,” which is more robust than “We gave lots of drugs, including sugammadex, and there definitely was anaphylaxis.”
There are suggestions that the incidence may increase over time. We might see an increase as more and more people are exposed to sugammadex multiple times, and the fact that cyclodextrins are found as food preservatives and drug carriers and in other products where you might end up inadvertently being sensitised to one of the structures that just so happens to also be found in sugammadex.
Contextualising the Anaphylaxis Risk
31:05–32:37
- Teicoplanin: most anaphylactogenic drug routinely used in anaesthesia, at approximately 1 in 6,500.
- Teicoplanin should be given slowly (1–2 mL at a time, or in a bag) rather than rapidly.
- Caution: reconstituted teicoplanin mixed with gentamicin precipitates instantly and resembles propofol – a drug swap hazard.
But let’s contextualise this, because no one likes anaphylaxis. There are other drugs we give that are far more likely to cause mischief. Teicoplanin is the most anaphylactogenic drug we routinely use, at one in six and a half thousand incidents of anaphylaxis. Now, that was pulled from a paper referenced in the show notes.
We give teicoplanin all the time. I know, hopefully now that we’re all giving it quite hecking slowly, as opposed to just boshing it in. When it’s in a 20 mL syringe, it’s easy to give a bit too much at a time. Really you should give one or two mLs, do other things for a bit, one or two mLs, do other things for a bit, or stick it in a bag.
But if you want to create an accidental syringe of something that looks like propofol, draw up teicoplanin and then draw up an ampoule of gentamicin into it. I did it this week just to see just how quickly it precipitates, and in a flash it turned white and looked like propofol in my 20 mL syringe. I discarded that and I was quite amazed at how rapidly it precipitated. I’d like to do the same with dexamethasone actually. Because when you’re giving the teicoplanin, it gets blooming annoying because you’re like, “Oh, there’s teicoplanin in my IV line – I can’t mix that, or I can’t mix that.” And routinely I split my gentamicin dose. I give a bit and then do some other stuff and then I give the other bit as well. It’s just awkward. Anyway, getting ahead of myself – we will do teicoplanin in the future.
Can Sugammadex Reverse Rocuronium Anaphylaxis?
32:43–34:44
- The jury is out: case reports exist both for and against efficacy.
- Some case studies report improvement, occasionally requiring a second dose to mop up residual rocuronium.
- Other case studies report no benefit.
- Anaphylaxis is not a singular event – mast cells release serotonin, bradykinin, and other mediators triggering vasodilation and endothelial changes.
- Treatment often requires prolonged adrenaline infusion (e.g. ITU admission, BP lability over 6–8 hours).
- Given revised incidence (~1 in 24,000), reasonable to try sugammadex during suspected rocuronium anaphylaxis.
Can we use sugammadex to reverse rocuronium anaphylaxis? I think the jury is out, because there are certainly case studies which say, “We had anaphylaxis to rocuronium. We gave sugammadex and everything got better.” A number of these case studies say everything got better, everything got a little bit worse again, and they gave a bit more sugammadex and everything got better again. Because you need to mop up all the molecule, otherwise there is molecule tickling mast cells.
I have been in a situation with a rocuronium anaphylaxis. It’s not the first thing you reach for, sugammadex. It took maybe 10–15 minutes before we thought, “Shall we give it a go?” It didn’t really do anything. I think in part it could be that it wasn’t the rocuronium, but I think later allergy testing demonstrated that it was. And in part, it’s not just a singular pathological event, an anaphylaxis. It’s not just “Here’s some histamine, off you go, once the histamine’s out of your plasma, it’s all tickety-boo.” The mast cells produce serotonin, bradykinin – these things trigger vasodilation, other endothelial changes that lead to an extensive process.
If anyone else has treated anaphylaxis, you don’t just give one bit of adrenaline and it all magically goes away. It peters out over time. And that patient ended up on ITU on an adrenaline infusion as their blood pressure lability slowly eased over like six to eight hours. But other case studies have said, no, it didn’t work.
I think when we thought there was a one in two and a half thousand chance of causing anaphylaxis with sugammadex, people were rightly slightly cagier about it. I think having read the truer incidence, I probably would just reach for some sugammadex and see if you can make it all better. Presumably at that point though, you do have the patient intubated, so you can control their breathing regardless.
Summary
34:44–36:12
- Sugammadex (Bridion): modified gamma cyclodextrin; one of the first selective relaxant binding agents.
- Encapsulates the steroidal ring structure of aminosteroid NMBAs in its hydrophobic cavity at a 1:1 ratio.
- Renders rocuronium biologically inactive, creating a concentration gradient drawing rocuronium away from nicotinic receptors.
- Dosing: 2 mg/kg (fade on TOF), 4 mg/kg (deep block, PTC 1–2), 16 mg/kg (rescue reversal).
- Kinetics: no protein binding, no metabolism, renally excreted, 1.8-hour half-life.
- Side effects: anaphylaxis (~1 in 24,000); oral contraceptive interaction.
- Flucloxacillin can displace rocuronium from sugammadex – wait 15 minutes.
- Do not re-paralyse with rocuronium after sugammadex – use atracurium or suxamethonium.
So in summary: sugammadex, Bridion, is a modified gamma cyclodextrin. One of the first selective relaxant binding agents. It works by encapsulating the steroidal ring structure of the aminosteroid neuromuscular blocking drug, holding it inside its hydrophobic cavity at a one-to-one ratio. This renders the rocuronium biologically inactive, creating a delightful concentration gradient between neuromuscular junction and plasma that draws rocuronium away from our nicotinic receptors on our muscle.
If you can see fade with your train-of-four, give them 2 mg per kg. If you can’t see fade but you have 1 to 2 post-tetanic twitches following tetany, give them 4 mg per kilo. And it’s 16 milligrams per kilo for rescue reversal.
Kinetics-wise, there is no protein binding, there is no metabolism, it’s renally excreted, 1.8-hour half-life. Bar the anaphylaxis, its side-effect profile is dreamy, but remember oral contraceptives are an issue. And flucloxacillin has fabulous philandering abilities when it comes to tempting that rocuronium out of the clutches of sugammadex. Don’t try and re-paralyse your patient with rocuronium if you’ve given them sugammadex. You need to be reaching for atracurium or sux. They are likely to work more quickly. Beautiful.
Outro
36:12–37:29
Thank you everyone for listening to this Good Friday episode on sugammadex. I know we’ve been venturing off into the long grass with vecuronium and pancuronium, and I thought bringing it back to reality to close out our paralysing drugs chapter just tied things over nicely. Take a moment to say thank you very much for listening. 100,000-plus listens, 2,000-plus direct followers. Never thought it would get this far. I just thought it’d be fun to do a podcast. So thank you very much.
Ahoy, Team Anaesthesia! You’ve survived yet another episode of Gas Gas Gas. Now if you’ve found it useful or harrowingly awful, please like and subscribe. Drop us a star or twelve and follow with whichever podcast platform you find yourself using. Please leave a comment or ping off an email if you think I need to square something away. Now there are a bunch of ways to support the costs of Gas Gas Gas, from buying me a coffee to venturing forth via an affiliate link to the horde of joyful SBA questions from Teach Me Anaesthetics. Those links are on the website and in the show notes. Speaking of website, definitely check out gasgasgas.uk for the show notes, diagrams, details, the references.
Now we all know, guys, that this is a bucket of content to consume and it is like drinking from a fire hose. So I want to finish by saying: take it day by day. Don’t overcook yourself, don’t freak out, and keep studying.
Enjoyed this? Review on Apple Podcasts Rate on Spotify
Support the show Help keep the lights on SBA question bank @ Teach Me Anaesthetics