
Poly-Compartmental Confabulations, The Rubber Ducky Effect Site and more.
This episode and post pairing will have you talking multi compartmental model pharmacokinetics like a champion in no time.
Article Spring Board
How do compartment models explain drug distribution?
Compartment models simulate how drugs distribute and eliminate in the body, using mathematical representations to predict concentration over time in different body compartments.
Quick Overview of Concepts
Volume of distribution is heavily dependent on lipid solubility - but the quoted VOD of drugs is only for single compartmental models - there is a VOD equivalent for each individual compartment.
Multi Compartment Models contain:
- Plasma
- Good blood flow compartment
- Poor Blood Flow compartment
- Sometimes have an Effect site compartment if that is what you're aiming for
- Considers clearance to only occur from the plasma compartment.
- Constants which dictate the rate of shift between these compartments and the plasma compartment.
The Main Topic
A single compartment exhibits straightforward kinetics, often described with simple 3 variable formulas,
Often with a single rate of clearance, a specific half life and a defined space which is filled (volume of distribution)
We have to start thinking about things in less convenient ways. If you’ve a pint glass full of beer, you drink it at a different rate compared to a shot of sambuca or a measure of Raki….
(start to imagine here, that the concentration gradients, initial plasma concentrations start to lead to different curves on your concentration/time graph (but with alcohol its zero order kinetics so fixed rate clearance which is not the norm.) )
We've mentioned Log concentration/time graphs before and thats what we should be thinking of from now on for these kinetic concepts.
We've spoken about drugs being more or less lipid soluble, and how their clearance behaves depending on how much drug is available in the plasma.
The plasma is a compartment, and is the critical avenue agents re-distribute in and out of around the body, and perhaps the only really true pharmacokinetic compartment which has a physiologic and anatomic counterpart - the rest are just a bit of a fudge.
To create a truly anatomically / physiologically reflective model would:
1) Be mathematically complicated
2) Hard to truly ever define, because you might decide that different parts of organs should have their own compartments depending on their relationship to blood flow etc how far do you go?!
3) Probably wouldn't yield any added practical value to delivering TIVA and other modifications to how clinicians use it would likely be better. (like dialing up your own bolus/time at the start + effect site target at ~5 mins and the model adapting)
Diffusion
Thickness, molecule size, molecule solubility are all important.

Dynamic Equilibrium
We have also mentioned the concepts of alpha and beta half times – ie the plasma redistribution phase in half-time parlance and the elimination rate from plasma respectively. Which reflects reality a little more closely.
While these are looking at decay over time, it doesn't factor in that agent is shifting constantly between compartments, in and out of tissues.
There are many factors that govern this dynamic equilibirum: solubility, blood flow, clearance, protein binding, receptor affinity, presence of other agents that displace the one you're interested in. All marvellous, all a very deep dive for boffins in laboratories, not us.
So we're going to go on a journey, of hyperbolic practicality to really imagine what on earth is going on. And then we will bring it back down to the peck and hill reality of squares on paper.
If we then think back to our dear buddy fentanyl we know that if you infuse plenty, over a very long time, you fill the patients lipidtastic proverbial great lake – (the Caspian Adiposity). The escape from this lake will differ from the wash out from their muscles / solid organs.
In this slightly hyperbolic patient situation we will presume that the patients Caspian adiposity is almost more fentanyl than fat at this point, we will suggest that if we were to continue any longer we would have put so much fentanyl into them that we were about to overwhelm all of their tissue compartments and start hypothetically stacking it up in their plasma. May their goblet overflow with fentanyl.
So if we are measuring plasma concentration over time, we would see on this journey to filling them up an initial Conc/time graph which will either have diminishing conc, if our infusion rate is too low, or a climbing conc as our rate is sufficiently high.

If our infusion rate was very high, we would reach peak clinical effect quite quickly, and on cessation concentrations and effect would rapidly diminish.
We are trying to fill our patient up, to achieve this, the fixed infusion rate, at the very least must exceed the patients renal/hepatic clearance mechanisms, if we were only just above this rate, we will be waiting a long time, but we will eventually get there.
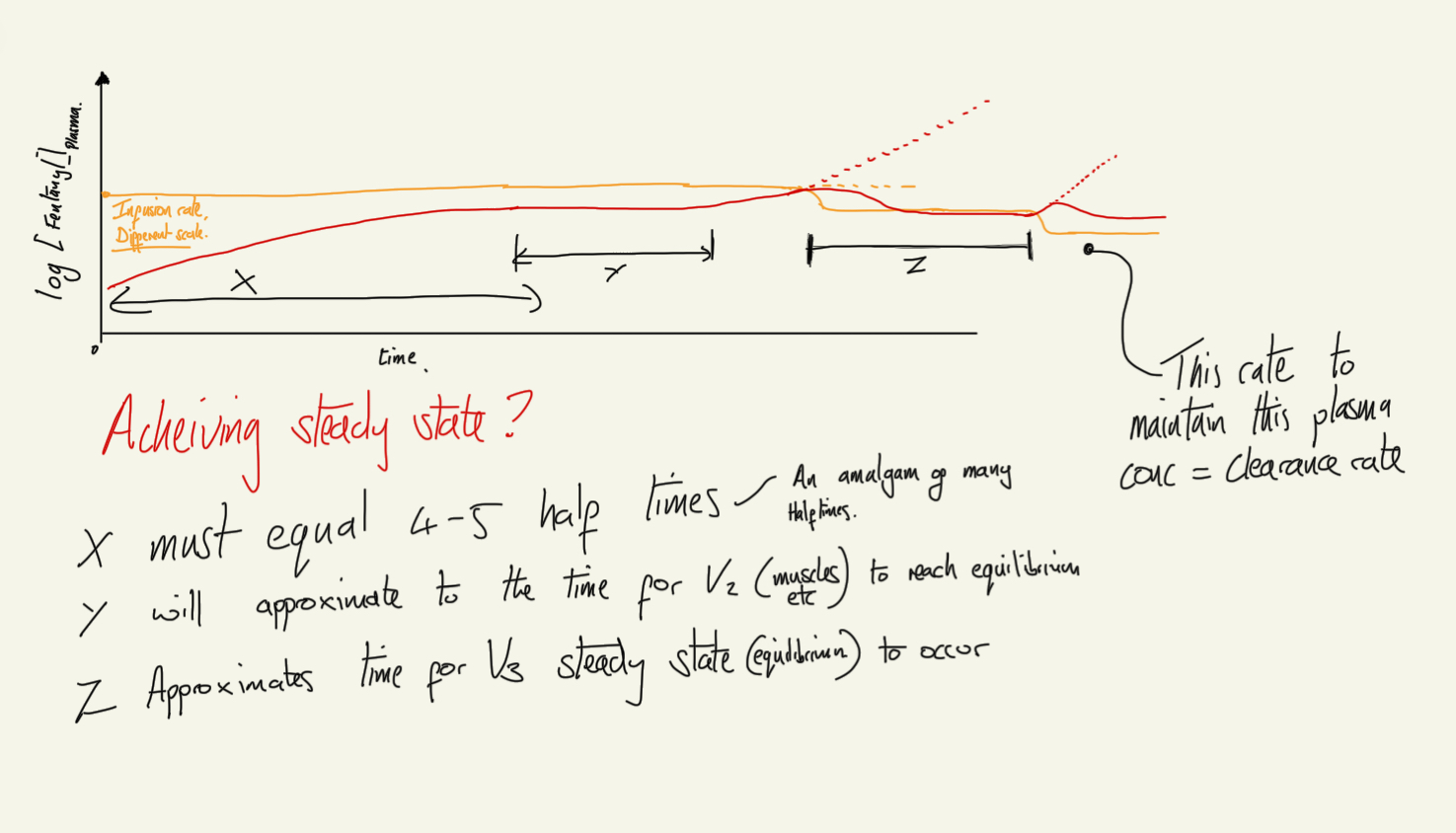
So we are going to start our rate in the middle and aim to keep the plasma concentration steady, and go and drink tea for the many many half times that need to elapse for us to fill them up.
Eventually, our steady state will wobble and begin to climb, the patient might be saturated!
We should fiddle the rate down, and achieve a new steady state, as it may be that there is more space in the fat, but our infusion rate was slightly to high for the rate of uptake for fat +clearance mechanisms alone.
More tea, more time
The concentration begins rising once more - now we are saturated.
To maintain steady state at this point, we would need to match the rate of clearance only. So we shall, and we could go drink tea indefinitely and this simplified system would stay steady.
If we were to decide to aim for a high plasma concentration at this point, we would have to go through the same process again, as we would need to achieve renewed dynamic equilibrium between these compartments.
But now we are going to stop.
On the cessation of the fentanyl infusion,
A negative trend begins, and the process goes into reverse,
A decay rate in fentanyl that reflects the rate of liver metabolism and renal excretion is present, which itself is limited by plasma drug availability, in turn limited by the rate of shift of fentanyl from these multiple differing tissues, governed by all the factors discussed above.
In our hyperbolic human we might get tempted to think that the concentration gradient is going to be rather high as we have infused most of the hospitals fentanyl supply into them, but we must take into account the 'theoretical' space which the fentanyl is in. If that space is theoretically rather massive then the concentration within that space of fentanyl will reflect that of the plasma at point of equilibrium.
First Concentration:Time graph of Fentanyl
If we had a patient with no liver or kidneys.
It would drop to a new equilibration point where by the flow of fentanyl into plasma from compartments and flow from plasma into compartments was nearly even. Governed by the time it took to reach a steady state (4-5 half lives) betwixt the varying uptake and decay constants of these compartments.
Naturally our patients fentanyl plasma concentration will in fact decay because our patient is not in such a sorry state.
Another thought experiment
If the trickle of fentanyl into plasma is very slow And the Metabolic Moppery was very efficient you would have a situation where the patient might stop experiencing new opiate receptor agonism as the fentanyl decays away from effect site and can't make it back
This situation wouldn't occur given that there are two organ systems which clear fentanyl, and they do not recieve the whole cardiac output meaning some drug from muscles/fats will squeak their way toward brain
I imagine that the closest you might get to this situation playing out is those drugs in which the plasma itself gets busy with clearance Ie Suxamethonium and Remifentanil (psuedocholinesterase and esterase respectively). It would have to be near instantaneous clearance of what ever becomes available in the plasma and in reality it would never truly technically occur. (I am also imaging that a mere technicality of diffusion of fentanyl from the early end of the capillary bed into blood with less fentanyl in it, vs the distal end of the capillary bed, which might have less fentanyl in the tissue then the blood thus returning agent to effect site unless plasma clearance can drop the concentration sufficiently across the time it takes to move along said capillary bed.) - I apologised in advance, does anyone know the answer to that?
Back to the main thrust of it all,
We have turned off the fentanyl tap.
Clearance is such that the patient will allow the fentanyl to slosh around the plasma looking for its next home, some will be mopped up by the liver/kidneys but some will totter off in the direction of the target site.
Derived from the shift into plasma from the vast lipid store- which will maintain a reasonable plasma fentanyl concentration.
Returning to our graph of fentanyl concentration at the cessation of infusion, its dipped off as we turned off the tap - this tap was maintaining a fair steady state in the plasma.
Our system undergoes turbulence as this change requires a new steady state to be sought,
the waves of equilibration of settle out - but as we know clearance is ever present, our system will never return to a steady state, and will equilibrate slowly towards emptying.
Ive decided that an analogy to all of this might make it easier to remember and more fun to talk about, so im going to introduce you to the Rubber Ducky Effect Site, and its pals.
You heard it here first - and i'm going to explain this.

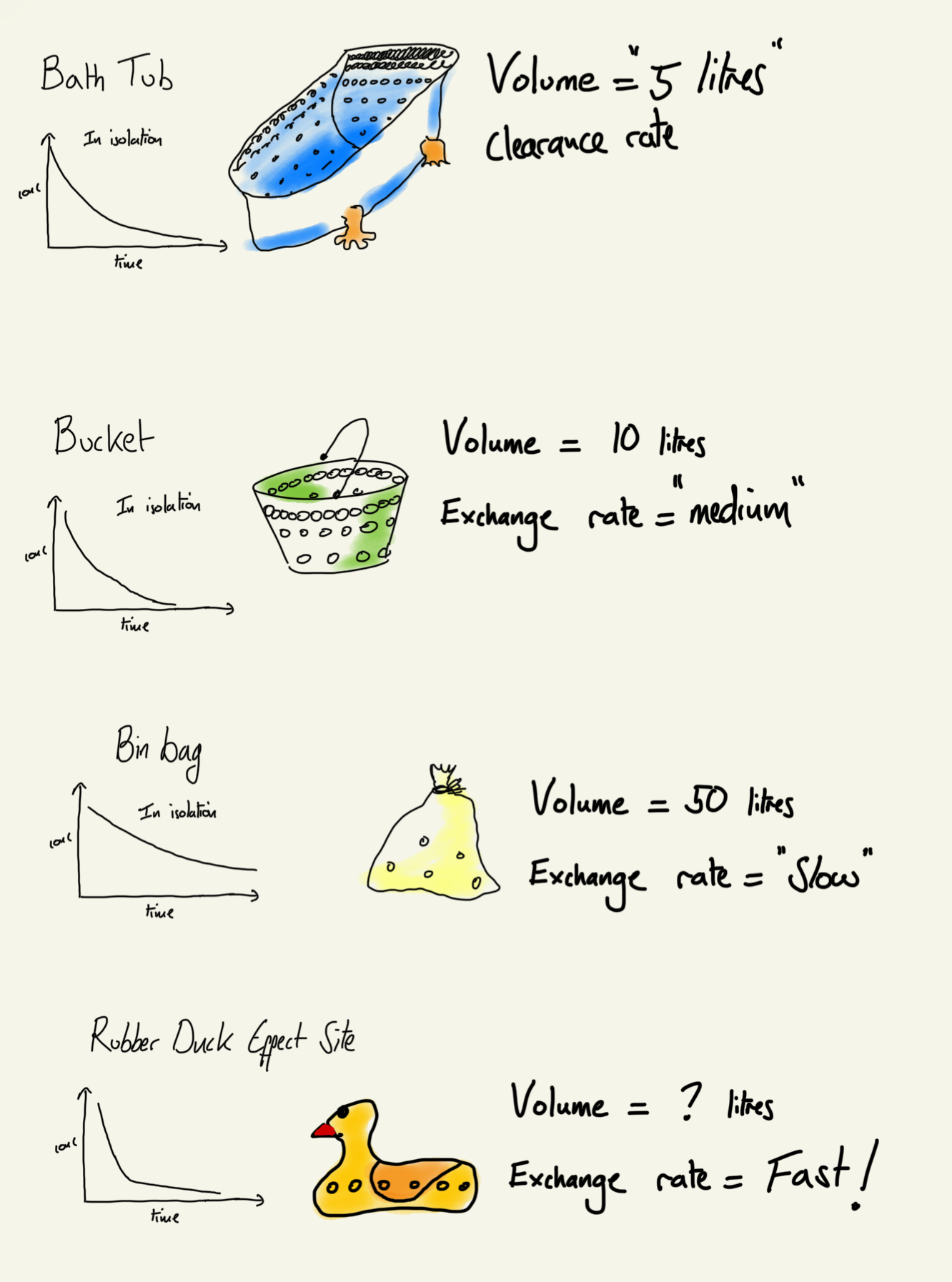
Bathtub
We will imagine that we've a bath tub, full of 'plasma' on the sides of the bath we have rings and rings of small holes, many many holes (we will say 1000) near the top that let fentanyl out, but as we track down the sides of the pool, the number of holes diminishes and the rate of reduction diminishes. Ie bathtub first order kinetics.
Bucket
We will also put a bucket in the bath tub 100 holes in it in a similar diminishing manner. And chuck a similar concentration of fentanyl in that.
Bin / Trash Bag
We are going to make our bathtub more complicated. By adding a bin bag of fentanyl (the tissues that are less perfused) with say 10 holes in it. With that similar diminishing manner (as concentration goes down, the rate of shift from the space drops off too)
And now that all goes in the bath tub,
So we have two ‘compartments’ that communicate with the plasma bathub of holes but each compartment could also pass agent via the main bath tub to the other.
For the sake of PK models in pumps, im going to add a ‘Rubber Ducky Effect Site’
The RDES has a semi theoretical volume and a number of holes which are guessed at, because as we know, it is not cricket to do brain biopsies to ascertain effect site concentrations of agents after sufficient fixed periods of infusions because that is unethical.
The rubber ducky of uncertain 'buoyancy' also exchanges fentanyl in and out of it, and is generally very well perfused and is considered to be quick to get to equilibrium with the plasma concentration.
This seems all a bit mad.
But it illustrates that we have four compartments, all having a rate of interchange between them via the systems central plasma (bathtub compartment) And that if left to empty of their own devices, they have particular speeds at which they could empty.
Remember, the central plasma compartment is where the clearance occurs.
Returning to our plasma fentanyl concentration person
We've seen equilibration, to a new gradient on the curve that reflects the shift of fentanyl from well perfused organs to the plasma and a smaller fraction from the less perfused fats and bits, Remember it is a fraction of this which gets cleared (out of the bathtub).
Everything will diffuse down concentration gradients – (there is no notion about active transport across membranes in these models, even if their was - in reality if you measure concentrations and their shifts overtime between spaces over time, you don't really need to know how it is shifting, only that it does.)
If you were to stop the metabolism/clearance, then a new steady state would equilibrate throughout the compartments and not much would happen.
These rubber ducky effect site concentrations will align to the plasma concentration At steady state.
So, we've been observing this patient for quite some time, and noticed out concentration:time curve initially barely dropped on cessation of drug, as it is now reliant on clearance to dictate the decline, if there was a lack of equilibrium in other compartments on cessation, then you would have seen a sharper decline as agent equilibrates.
Remember;
Remember; we stopped the infusion at the point where the concentration of fentanyl in our human overall matches the lipid stores concentration - (the fentanyl bin bag in our analogy).
We should imagine a threshold at which the rubber ducky effect site experiences a clinical effect be that side effects or clinically intended effects, and that different concentrations will bring out more or less of these, and side effects may appear at different concentrations to clinically useful effects.
Having stopped the infusion, the muscle compartment bucket and the bin bag have the opportunity to empty its smaller fentanyl store - but do recall that its relative concentration is very near to plasma concentration (which is slowly diminishing since stopping infusion) so its capacity to shift out is also slow. If there was a sudden drop in plasma concentration to zero, then the speed of shift would escalate

Note this rate is decelerating as the concentration goes down (see Michaelis Menten Kinetics Hepatic Clearance podcasts).
Its relative concentration is similar but its blood flow ie shift out is slow, as it squeaks out of the fat it may end up being taken up by other compartments.
At this point you can imagine that the descent of this graph to zero is going to be quite long (and technically never gets their/ due to half lifes / asymptote things etc). And that the concentration in the plasma, and thus amount available to clear is going to be on a negative trend - the rate will be decelerating.
There is a threshold here at which your rubber ducky might not exhibit a clinical effect, but it is worth considering that the effect site concentration to achieve a side effect of a drug might be different to that of the clinical effect you’re trying to achieve.
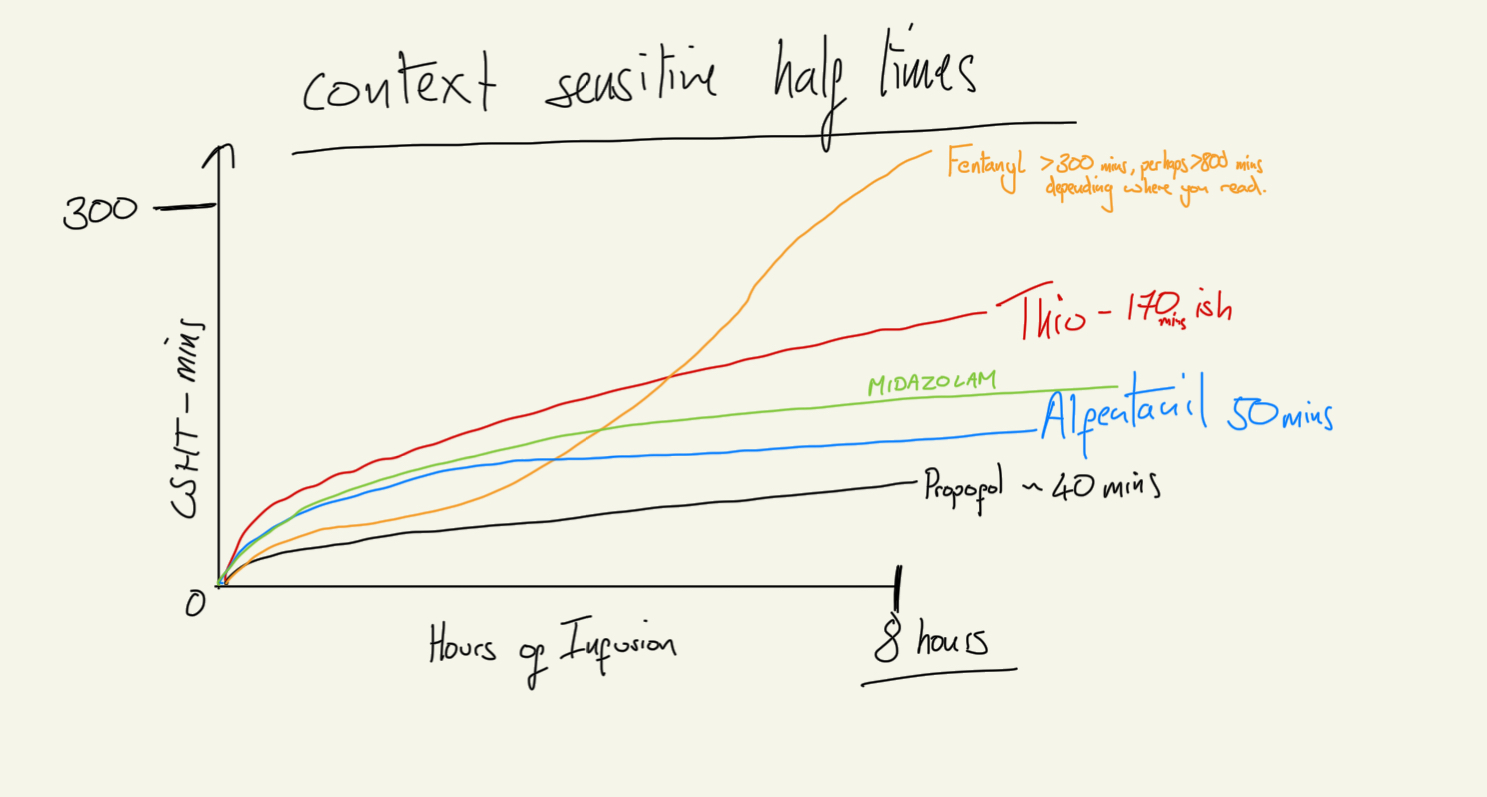
Recall that fentanyl half life is 141 (2.3hrs) – 853 (14 hours) mins in studies, is 10% renally cleared and cyp3a4 enzymes get busy converting it to nor-fentanyl and its other metabolic buddies.
All this thinking about compartments can get boiled down to context sensitive half times. - which we have maxed out in our hyperbolic fentanyl filled fantasy.
CSHT
To shift this rubber duck madness into FRCA compatible dialogue there are some terms to know:
Compartments
Plasma bathtub = C1 or V1 – The central compartment.
Well perfused Bucket = C2 or V2 = The vessel rich compartment.
The barely perfused bin bag = C3 / V3 = Vessel poor store.
Rubber Ducky Effect Site = Ce / Ve
Interchange Co-Efficients
K12 – Rate of shift from V1 into V2 (Bathtub to Bucket)
K13 – V1 > v3
K10 – Central Compartment Clearance
And this Nomenclature also works for the rate of shift out of for example V3 into V1 as K31

Summary
To summarise we have described the journey fentanyl takes through a human, exploring a few different extremes in the example to illustrate key points (clearance, dynamic equilibrium and volumes of distribution). Multi compartmental pharmacokinetics play out with all drugs, but we just happen to think about these ones as anaesthetists. I imagine that the microbiologists are tempted to think about the abscess, the brain, the lungs as compartments that they are targeting.
- Understanding the shifts between these compartments is something you already think about when using volatile!
- If you're getting to the point where they are asking you to draw out the formula to calculate current plasma concentration for a multi compartment model you are doing just fine
- Remember that all these things are occuring at the same time and are not linear, and that there is a reason why a computer in a pump is doing it and not you with a bit of paper
- You could, choose to use TCI as a black box, presuming that with sufficient targets your patient will be asleep, and if they are wriggling they are not deep enough, and not get too het up with the minutiae. The only problem with that, is that the models are still not perfect - and if you arent careful you can easy over or under do it.
- Check out this TIVA simulation APP and have a play - its cool.
If you thought this was a worthy post and made sense - let me know and click email Dr Gas Below!
"Thanks for listening guys... Every day you are getting better at this. Take it day by day, don't overcook yourself, don't freak out, and keep studying!"
Podcast Information & Support
Support the Show
Contact & Feedback
- Comments: Share your clinical experiences and ask questions!
- Corrections: Help us improve accuracy and clarity
Follow GasGasGas On
- BlueSky:Gas Gas Gas (@gasgasgaspodcast.bsky.social)
- X / Twitter: GasGasGasFRCA (@GasGasGasFRCA) / X
- FaceBook: Facebook - Gas Gas Gas
- InstaGram: GasGasGas
Transcript
Gas Gas Gas: Polycompartmental Madness Part 2
Introduction and Series Context
00:00-01:12
Hello, everybody, and welcome to Gas, Gas, Gas. I'm hoping that this is either the final or penultimate jaunt in the Polycompartmental Madness series that we've been experiencing. This is the culmination of a multitude of podcasts prior discussing half-lives, time constants, natural logs, but also hepatic clearance, volumes of distribution, in order to try and get ourselves to a point where we can really appreciate using the tools and pharmacological knowledge at our fingertips to understand how a drug shifts through a human being.
This episode has been in draft since before Christmas as I've tried to determine the best way to tell you all about these crazy things. You'll have to tell me what you think and whether or not I need to wind my anecdotal analogies in a bit. [email protected] is the email address, because I totally appreciate that the next twenty to twenty-five minutes of your life are going to be a wild ride, but hopefully at the end of it you'll be like, "oh yeah, this lunatic does actually make sense, and has brought it back to reality."
So we will return to reality by the end of this episode, depending on what you think reality is, everyone.
Multi-Compartmental Model Basics
01:12-02:45
First up, let's just remind ourselves that volume of distribution is fairly reliant on the level of lipid solubility. The quoted volume of distribution for a drug reflects that single compartmental situation, but it's important to think that a volume of distribution also ties to a particular compartment - how readily a drug could dissolve into the fat compartment, for example.
I'm going to tell you that most multi-compartmental models have a mix of a plasma compartment or a central compartment, a compartment that receives good blood flow, a compartment that receives poor blood flow - the comparisons here being muscle versus fat - and they sometimes have an effect site compartment, which is the area you're aiming to get drug to in order to exert clinical effect.
These drugs generally only consider clearance to occur from the plasma compartment. Seems very reasonable, and these models have a multitude of constants that reflect the shift of agent between these compartments and the central compartment.
It's important to emphasise that single compartment kinetics make the maths easy and convenient, often being described with those simple half-time volume of distribution clearance formulas that we've mentioned before. But unfortunately, simple doesn't mean correct, and even complicated doesn't really mean correct either, but we have to start thinking about these things in a less convenient way because the exam would like us to, and we should probably think about it just for our day-to-day practical work.
Alcohol Analogy and Central Compartment
02:45-04:26
So first up, if you have a pint of beer, a glass of wine, and a measure of sambuca, you're going to consume these at all different rates. That means the plasma concentrations of these drugs are all going to occur at different rates with different peaks. That means the graphs of these three different agents will look different.
Now if we lay those curves on top of each other, it might start looking a little bit like a graph that reflects the shift of agents through multiple compartments having been introduced to a central compartment. This central compartment is key and is often defined along with the other compartments by the weight, height, age and gender that you put into these models.
Interestingly, this central compartment, or plasma compartment, is likely to be the most anatomically relatable to a human compared to these other ones, because we can theoretically measure how much plasma someone has, although again, I don't think anyone would be terribly impressed if you were to do it.
Counterposed to that, the other compartments are quite a little bit more theoretical and they do not reflect a specific set of tissues. You could seek to develop a model that was anatomically physiologically more reflective - it would get exponentially more complicated as the interplay between all these compartments went about their business. But also, you can imagine this would be deeply challenging because you might start thinking that different parts of organs receive different amounts of blood flow and therefore would have to be reflected differently.
This could go on forever, and ultimately it will fail to be of any clinical use. And that is why we have these moderately fudged compartments that approximately reflect the average volume, blood flow, kinetics of pharmacologically and physiologically relevant bits of a human.
Factors Governing Compartment Shifts
04:26-05:59
I think we'd all be much better off if someone would be so kind as to set up a model where you can program in the bolus you reckon you want to give, and over how much time, with an effect site target of your choosing at perhaps two minutes or five minutes in order to avoid that kind of slow, dozy, doze off to sleep and prevent you from having to just bolus a propofol and then start your TCI, which, you know, on paper means that you don't truly know what your effect site is. You can presume it's probably marginally higher.
But then the important thing is to think about what factors govern the shift of agent between these compartments, because clearly we have to have appreciation of that first.
When thinking about this interplay, you need to consider the molecular weight of the drug given. Big stuff doesn't get across membranes as much as small stuff. The molecule solubility, blood flow, the clearance, the protein binding, the receptor affinity in your effect site compartment, and the presence of other agents that might displace the one you're interested in from where you're aiming to go.
It's important to have a notion of these, but unless you're going to be the next Schneider, don't worry about it too much. Just appreciate that Fick's law of diffusion plays out here just as much as elsewhere.
The Caspian Adiposity: Fentanyl Example
05:59-09:04
So now for the main thrust of it all. Buckle up, locate some coffee, maybe read the show notes first, and my dearest apologies in advance for the unusual journey we're going to take.
So we need to think back in our minds to a previous podcast on fentanyl, because that's the example we're going to use here. And we know that if you infuse plenty of fentanyl over a long, long period of time, you will fill the patient with fentanyl.
I'm going to try and convey the size of this lipid compartment we're going to play with to you and say that it is the size of the largest lake in the known world, and that's actually the Caspian Sea. We're going to call it the Caspian adiposity.
In this slightly hyperbolic patient situation, we're going to assume that we've trickled fentanyl in for such a long period of time at greater than the rate of clearance that we have filled this Caspian Sea with fentanyl, and that at the concentration we're aiming for in their plasma. If we were to give them any much more, that plasma concentration would start creeping up as we've almost fully filled that plasma compartment at that concentration. May their goblet overflow with fentanyl.
So now if we are thinking about measuring plasma concentration over time, we could think about how this journey to filling them up goes. The crux here is that you would need to infuse fentanyl at a rate faster than the liver and kidneys were eradicating it from the system. Lower than that, you will never fill the patient. Higher than that, you will begin to fill the patient.
The other dictator here is do we want to see a clinical effect, and how quickly do we want to see that clinical effect? If we were seeking to see it promptly, we could either start a fast fixed infusion rate, therefore ensuring that we achieved higher plasma concentrations and subsequently higher concentrations in the brain where we're aiming for, or a bolus and then a slower rate of fixed infusion. And remember, we're trying to fill this patient with fentanyl.
Steady State and Compartment Saturation
09:04-11:34
If we were to just give that bolus though, remember, we would hit high concentrations in the central nervous system very quickly, but they would rapidly redistribute and your clinical effect would disperse.
For the sake of our hyperbolic Caspian patient, we're going to aim for a fixed rate of infusion that surpasses hepatic clearance and renal clearance. And we're going to allow it to reach a steady state. It doesn't have to be a specific concentration quote here. Just imagine I started an infusion, four to five half-times have occurred, and we're now at a steady state in that plasma.
So if we imagine our graph of log concentration on the y-axis and time in linear on the x-axis, we've started our infusion, and we've seen a slow upward incline that has levelled off as a steady state of fentanyl in versus fentanyl out - and when I say out, I mean out of the plasma, not out of the patient entirely - has occurred, and we are cruising at a steady state. And the patient might be experiencing some pain relief and being quite happy about this at this point in time.
And now we're going to watch, and we're going to watch and watch and watch some more as this seemingly steady state continues until it begins to climb. What has happened here is you've likely achieved saturation of one of your compartments, the more readily perfused compartment. At that point, we'd have to turn our fixed rate infusion down, try and figure out exactly where we want to be to return to our steady state.
We're now achieving the same concentration and subsequent effect in the patient, but we're giving a lower rate of infusion. More time passes - might go drink a cup of tea, go have some fish and chips - and then we notice our plasma concentration begins to climb again. We've now saturated the less readily perfused compartment, the Caspian adiposity.
We have to titrate our fentanyl right down even further at this point to achieve a return to that steady state. At this point in time, your infusion rate is actually going to reflect the hepatic and renal clearance rate in this system. This is truly where you might find your patient in a steady state for an exceedingly long period of time, unless something were to physiologically change with your patient - you improved their clearance, you impaired their clearance.
Equilibrium and Concentration Gradients
11:34-13:50
And here we are at an interesting place, whereby the concentration of fentanyl in this human is fairly homogeneous across their plasma, their central nervous system, their muscles, their organs, their fats - all more or less the same, or frankly exactly the same concentration in these separate compartments.
Now it's important to think about the fact that these separate compartments have differing volumes of distribution. So if you've got a very capacious compartment like the Caspian Sea, you can fit loads of fentanyl in there before you'll start to meet the concentration at which the rate of fentanyl going into the compartment matches the rate of the fentanyl going out of the compartment as you've achieved that dynamic equilibrium.
The difference here between a multi-compartmental human and a single compartmental human is that we might get tempted to think that the patient has a very high concentration gradient of agents not in the plasma versus in the plasma, but we must take into account the fact that it is in a theoretical space dictated by the lipid solubility and volume of distribution of that compartment, and at that equilibrium point there won't be a difference in concentration between these two compartments until - that is - we stop infusing the patient with fentanyl.
At that point plasma concentration goes down and a gradient forms, although it's not a gradient of amount of fentanyl in human versus amount of fentanyl in plasma because it's governed by the rates of clearance that we'll go over in a minute.
Hypothetical Extreme Patients
13:50-14:50
But first, a few hypothetical patients to really illustrate this situation. If at this point in time where we stopped our infusion of fentanyl, we also had a patient who suddenly had no liver or kidneys, then that amount of fentanyl is just going to stay in them. There's no way for it to get out, and they would just get stuck at that steady state, probably feeling quite relaxed, I imagine, sans their kidneys and liver, which I'm sure they'd be moderately concerned about.
If we were to take this to the opposing extreme of a patient whose metabolic fentanyl clearance skills are so excellent that it can clear fentanyl like Usain Bolt can run the hundred metre sprint, mightn't we find ourselves in a situation where the clearance from the plasma is so efficient that we suck fentanyl from our effect site and other compartments so quickly that the effects of the fentanyl are immediately curtailed, because no further agent couldn't possibly get into the central nervous system?
Now for fentanyl, this situation couldn't really occur, because even if the liver and kidneys were so remarkably effective, they do not receive the entire cardiac output. So some agent circulating in the plasma will dodge clearance and recirculate past the central nervous system. So it won't work for us in this way.
Real Examples: Suxamethonium and Remifentanil
14:50-15:55
But you may get closer to this situation in drugs in which the plasma is getting busy clearing the agent. And the two that spring to my mind here are suxamethonium and remifentanil. Suxamethonium is cleared by plasma pseudocholinesterase, and remifentanil by non-specific plasma esterases.
But we have to think reality is nowhere near as exciting as this hypothetical delight of something that can be eradicated in an instant, but remifentanil gets somewhat close with its nine to eleven minute half-time and its relatively unsaturable enzyme system. Read Michaelis-Menten show notes, listen to Michaelis-Menten podcast.
So returning to our polycompartmentalised fentanyl-riddled human, we know that in this situation, the shift into the plasma from the exceedingly vast Caspian adiposity, lipid store, maintains a reasonable fentanyl concentration in our human model. We know that the clearance is such that the patient will allow this fentanyl to slosh around in the plasma looking for its next home, and we know that some of it will be mopped up by the kidneys whilst some of it is tottering off to other places to reside.
The Bathtub Model
15:55-17:55
So here we go back to our graph of log concentration on the Y, time linear on the X, and we've turned off that fixed rate infusion, and our graph has started to tip down very slowly back towards zero. Check out the show notes for these graphs, by the way.
But now we've got to think about how these drugs are shifting through this human to get out and what their behaviour might look like. And for that I'm going to introduce some anecdote that we're then going to tie back to compartments.
I want you to imagine a bathtub, and this bathtub is the plasma, and in that plasma, as you well know, there's some fentanyl floating around. But now we're going to introduce holes to this bathtub, going down the sides - many, many, many holes at the top dropping off to fewer holes at the bottom. Only fentanyl can get out of these holes, and you can imagine that when there are many holes, quite a bit of fentanyl is cleared, but as you creep down that bathtub less and less fentanyl can escape as the fentanyl empties out of the human. This is a way to reflect half-life.
You've got to imagine a big bathtub, because now we're going to put a bin bag, trash bag, garbage bag, depending on your terminology - it's obviously closed at the top. It's a bit flubby, almost a bit fatty looking. And this is full of quite a large space. It's bigger on the inside than the outside, and it's only got a couple of holes in, and this too is full of fentanyl at the same concentration as our plasma was.
We're going to then introduce a bucket. This too is full of the same concentration of fentanyl as the plasma, and this too is inadvertently seemingly larger on the inside than the outside, but not so much as the trash bag, and it has more holes than the bin bag to reflect that it is more readily perfused. Things can move in and out of it more easily.
And the pièce de la résistance is a rubber ducky effect site. This is a rubber duck - other bathtub related toys can be used - with a further number of holes in.
Drug-Specific Clearance Rates
17:55-18:25
Remember, these holes in these compartments that allow shift of drug between compartments are drug-specific, i.e. some drugs move quicker than others, as we well know.
If you're struggling to imagine this - bathtub, bin bag, bucket, rubber ducky madness - take a look at the crazed diagram on the show notes.
If you were to imagine that you turn off the fentanyl fixed rate tap into this bathtub, and we know that there's a fentanyl clearance rate out of the bathtub, there's going to be a bit of turbulence occurring as the presumed rate of influx of fentanyl has stopped - things need to re-equilibrate.
The Rubber Ducky Effect Site
18:25-19:10
There's a bit less fentanyl in the plasma, so some of the fentanyl from the lipid store, the bin bag, has to ooze out. Some of the fentanyl from the bucket, the well perfused muscly store, needs to ooze out, and all has to do a bit of a wibble and a wobble. Imagine these are waves of equilibration occurring in your bathtub.
I'd like to caveat that our rubber ducky effect site is a confused little fellow because his existence, whilst clearly likely to be true, is deeply in question as to how big he is, how many holes the poor fellow has, and therefore in our system how buoyant the little rubber ducky fellow may be.
And this is because it is not cricket to infuse a drug into a human being for a long period of time, and then do a brain biopsy to find out how much drug is actually where you're interested. You could have even radio-tagged or other such crazy biochemical things, to see how much drug is in there and where it is. All not sport.
So we have to rely on our clearly existent but of unknown morphological significance, rubber ducky.
Clinical Implications: Bleeding and Drug Distribution
19:10-20:00
So imagining this mad model, you can now appreciate that fentanyl is going to want to shift around these multiple compartments using the bathtub as its means of transfer, and that each of these compartments has differing behaviours compared to its friends because of its different rate of perfusion and of what material is being perfused.
We know that everything diffuses down concentration gradients, and even if there were other forms of shift - remember we've got facilitated diffusion and active transport, channels, etc. - we don't really need to appreciate how the drug shifts, just that it does shift, and that with each change that you deliver to the system, it has to re-equilibrate.
So if we were to accidentally exsanguinate a patient, then we must think that we've emptied their plasma compartment. Perioperatively less of a concern if it's a heavily fat-soluble molecule, but more of a concern if it's a predominantly water-soluble molecule, because naturally most of that agent is going to be in your bathtub and only a scant amount in your bin bag or your bucket or your rubber duck, and therefore exsanguination is going to play a more pivotal role in the amount of drug in that human being.
This is perhaps why it's always a good idea to remember that if your patient is prolifically bleeding to death, whilst they may not need as much anaesthesia from a physiological perspective, don't forget that the amount of antibiotics in them has greatly diminished, and you might think about giving them an extra dose of those prophylactic agents.
Multiple Half-Lives and Steady States
20:00-21:55
So we have our rubber ducky effect site, and our rubber ducky is experiencing a clinical effect that is dictated by the concentration in our rubber ducky effect site. It's important to bear in mind that different concentrations might yield different clinical effects. You might see side effects from a drug, unfortunately, at a lower concentration than the intended benefits of the drug that may require a higher concentration to achieve.
Every time you titrate your drug to achieve an intended clinical effect, a new steady state has to bear out within your system. You create waves, remembering that it takes four to five half-times for a new steady state to form. But to make your brain hurt, there's a multitude of different half-times bearing out in this system when you make a change, because the rate of shift from plasma to bin bag is governed by its own constants - a constant for in and a constant for out.
Therefore, this re-equilibration is occurring across four to five steady states across a number of different half-times that are bearing out when you make that change.
So if we go back to our patient model, our slightly hyperbolic Caspian Sea, and we've turned off our fixed rate infusion, we are going to see descent of our curve. The descent of this curve is dictated by the clearance rate, but also the shift of agent back into central compartment from these external compartments.
If clearance was sufficiently high and rate of shift was sufficiently low, you might find yourself in a convenient place of being subclinical in your effect. Our patient stops feeling very relaxed, and their pain comes back. They're still full of oodles of fentanyl, but it can't exert its effect because its rate of shift is just too slow. That would be convenient.
However, it doesn't terribly bear out like that. And the effects of fentanyl linger for quite some time at the cessation of our very prolonged infusion.
Context-Sensitive Half-Time
21:55-22:35
This is what bears out when you're thinking about comparing the context-sensitive half-times of different drugs. Those with a high volume of distribution on paper and those with a prolonged half-time will subsequently have an exceedingly long context-sensitive half-time - a double whammy of bother when you're trying to get your patient awake, breathing and extubated on intensive care. And that's why in the UK you won't see a fentanyl infusion on ITU, really ever - there are better options out there.
Reality Check: Compartment Nomenclature
22:35-24:16
So you've imagined this bathtub of multi steady state, achieving ripples of equilibration every time you turn your infusion up or your infusion down. But we need to come back to reality because we can't just think about bathtubs and rubber ducks in the exam because we would thoroughly embarrass ourselves.
So to tie it all together, remember that our bathtub is in fact our plasma compartment. When you are looking at these models in schematic form on paper, in Peck and Hill for example, the central compartment is called C1 or V1. Our fairly well perfused bucket is the vessel rich compartment, or sometimes it's called the vessel rich group - this is C2 or V2. Our barely perfused bin bag is the vessel poor store, vessel poor group, C3 or V3. And our rubber ducky effect site is generally denoted by a big C little e or a big V little e.
In amongst all these compartments in this schematic form are the interchange coefficients - these are denoted by a k, k for constant, and then two numbers afterwards that reflect the shift from where to where. So from plasma to vessel rich compartment or from bathtub to bucket would be K12 or K bathtub bucket.
K10 reflects the clearance from the central compartment, the rate of clearance. That's because zero, or compartment zero, is considered the outdoors, the non-effective, the in your urine compartment.
Clinical Applications and TCI Systems
24:16-26:00
So I do terribly apologise for the analogy. I hope it makes some sense because it's really important to bear in mind that re-equilibration occurs, and steady state has to resume before you can really know how much of a clinical effect you're truly achieving with your drug.
If you look at your propofol TCI model as you dial up for the effect site concentration, it will actually overpressure the effect site by delivering a higher plasma concentration to try and get a concentration in the effect site you desire sooner. It doesn't want to overshoot, though, at this point, and it knows approximately what it thinks is the right amount to give.
Anyway, to summarise this journey through polycompartmental madness. It's important to understand the shifts between these compartments is something that you already think about when you're doing a volatile anaesthetic, so don't be terrified of TIVA. Just have a good read, do it with supervision, and accept that it seems really complicated, but in reality you're using a machine that just infuses propofol for you, giving you a hand.
Remember that between these compartments there's a lot of stuff going on and there's a reason why computers are doing it for us, so don't be terribly terrified by the formulas that you have to learn for the exam. The podcast before this provides an idiot's guide structure to barfing up that formula that you can almost write on the fly, depending on how many compartments they want you to talk about, because it's just the same thing repeated over and over, and you add them together to reflect each compartment.
Safety Considerations and Practical Advice
26:00-27:39
There's a link in the show notes to two applications - one, a TIVA simulator that's in a web browser, and then pointing you in the direction of a TIVA simulator on the App Store - both quite fun things to play with to get an idea of what's really occurring.
And I want to close out with: you could choose to use TIVA or the target controlled infusion pharmacokinetics software within a syringe driver as a black box. And actually, your clinical endpoint isn't a number on that black box, but it is if the patient is asleep or not, because that's what we're really after.
BIS, processed EEG, or the density spectral array that you get with that is very helpful. But one thing is to note: in that National Audit Project, I can't remember which one, looking at awareness, patients who were paralysed and TIVA'd were an order of magnitude more likely to have awareness than those who were not paralysed and being TIVA'd.
So only paralyse them if you have to, use short-acting paralysing agents and make sure that cannula site is okay. If it seems like you're using an incredibly large amount of propofol to keep someone who really doesn't need it asleep, then they're not getting all the drug you're giving them. Figure out why.
Conclusion and International Audience
27:39-27:39
That was a lot of talking. Thank you very much for listening. I'd actually like to say welcome to all the new listeners that are listening in over the last few episodes, especially you in India and Turkey and Sweden. I didn't think people would be listening from there. That's cool. If you like it, tell your mates.
And you in India, I've made sure to put the podcast on the Gaana platform. That should be live in a couple of days once they accept the RSS feed, just to make your lives a bit easier.
Anyway, my name's James. You've been listening to Gas, Gas, Gas, and I promise the next episode is not going to be quite so crazy.
Leave a Reply