Ep.46 – Sevoflurane For The FRCA Primary
12 November 2025
Contents
Having a solid understanding of Sevoflurane is, as you might expect, quite important for the FRCA primary and your career. as it is likely the most commonly used volatile anaesthetic agent, in the UK.
It might find itself adjacent to a Desflurane or Isoflurane vaporiser, and compared to these a few properties stand out, it’s the smoothest option for Gas Induction, it has the least offensive global warming potential, and has reasonable onset/offset (Desflurane is a winner here, however, polar bears are very allergic to Desflurane) and penguins are looking around for large walk in freezers, possibly due to its use.
This episode is part of the volatile anaesthetic agents series that kicked off with ‘an introduction to volatiles‘, and also an episode on isoflurane.
Sevoflurane Physico-Chemical properties
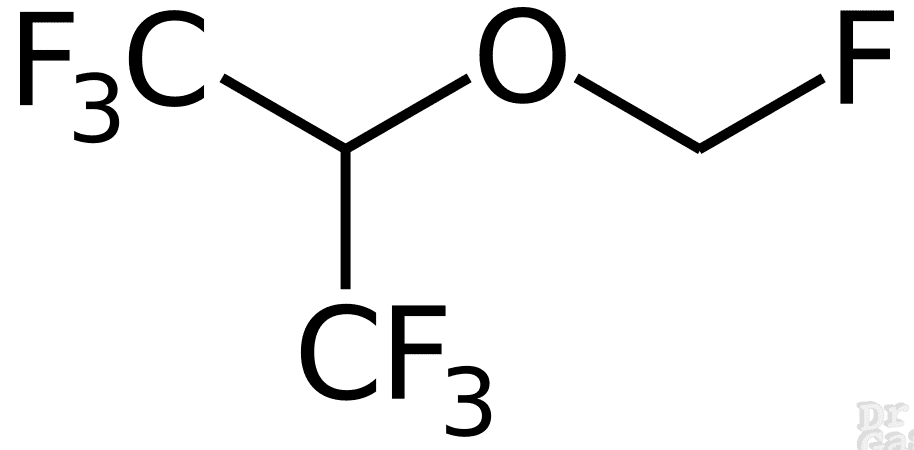
Sevoflurane is a polyfluorinated isopropyl methyl ether (C₄H₃F₇O), first synthesised in 1968 and introduced to UK practice in the 1990s; it is non-flammable, non-isomeric, and may degrade to Compound A in warm desiccated CO₂ absorbers.
| Name | Sevoflurane |
| Class | Polyfluorinated isopropyl methyl ether |
| Chemical Make Up | C4 H3 F7 O |
| History | First synthesised in 1968, Isoflurane was taken to market ahead of Sevo as it was considered the more likely successful agent. The rights to it was sold to Mariushi Pharmaceuticals which brought Sevoflurane to market in Japan in 1990 – Branded by Abbot Pharma in 1995 as ‘Ultane’! Generics were available from 2006 Flourine was generally an excellent atom to swap out with other peskier atoms in these volatile agents, Flourine chemistry was much improved courtesy of the Manhattan project |
| Isomer Status | nil |
| Colour/Appearance | Clear colourless liquid – Non-flammable |
| Stability | Degradation may occur via two pathways In warm desiccated alkaline CO2 absorbers at low fresh gas flows 1. Loss of hydrogen fluoride forming PIFE (Compound A) [pentaflouroisopropenyl flouromethyl ether] and PMFE (Compound B) trace pentaflouromethoxy isopropenyl flouromethyl ether 2. HFIP (See metabolism) and formaldehyde production > formaldeyhyde> formate and methanol . These can react with the above forming other irksome compounds (C,D,E) Or if the formulation was in fact dry as a bone – which it intentionally is not allowed to be Then a bottle of sevoflurane stored totally neat and in a glass/metallic bottle or exposed to aluminium in vaporisers, will do some janky madness with lewis acids found in the material of the flask and release hydroflouric acid. It will seek to erode and escape its container, exposing itself to more materials ( a source of Lewis Acids [any substance that accepts an electron pair]) Now, if the water content of the Sevoflurane is 100ppm it stops this, – Todays Sevoflurane contains 300ppm H2O as it is manufactured a bit differently, this very troubling problem. You would not want to fill a vaporiser with hydrofluoric acid and try and keep someone anaesthetised with it…… ( check out the anesthesia patient safety foundation here for the history of this! https://www.apsf.org/article/sevoflurane-the-challenges-of-safe-formulation/ |
| Molecular weight | 200g/mol |
Link to public domain file
Interacts with soda-lime at temperature of 65 degrees C – compounds ABCDE.
Are potentially toxic but never reach toxic concentrations
Isoniazid potentiates clearance
Sevoflurane for the FRCA primary
Key FRCA data: sevoflurane MAC is 2.0% in adults, blood:gas solubility coefficient 0.69 (conferring relatively rapid onset and offset), oil:gas coefficient 47, boiling point 58.6 °C, and saturated vapour pressure 22.7 kPa at 20 °C.
| Sevoflurane Boiling Point | 58.6°C |
| Sevoflurane Saturated Vapour Pressure (@20°C) | 22.7 KPa |
| Minimum Alveolar Concentration (MAC) | 2.0% (adults; 1.8% at 40 yrs) |
| Blood:Gas Solubility Coefficient Sevoflurane | 0.69 |
| Oil:Gas Solubility Coefficient Sevoflurane | 47 |
| ‘Safe’ Sevoflurane environmental Exposure | 20ppm (abbot) |
Sevoflurane Pharmacodynamics
Sevoflurane produces general anaesthesia primarily by potentiating GABA-A and glycine receptors and antagonising NMDA receptors; cardiovascular depression is dose-dependent via negative inotropy, and it is the preferred agent for gas induction due to its non-pungent odour.
| Mechanism of Action | Volatiles seem to disrupt synaptic transmission – especially ventrobasal thalamus Potentiates GABA-A and glycine receptors (positive allosteric modulation); may antagonise [NMDA receptors](/episode/ketamine/) (N-methyl D-aspartate) ‘Meyer-Overton’ – expansion of hydrophobic regions in the neuronal membrane either within the lipid phase or within the hydrophobic sites of cell membrane proteins ‘Gets around the CNS and causes mischief that renders people hypnotised, amnesic and generally less mobile’ |
| Chief Effect / Actions | Hypnotic |
| Dose | See End Tidal Mac for Dosing |
| Side Effect Profile | |
| Cardio-Vascular Side Effects | Chronotropy : No effect on HR Inotropy : negative effect – dose dependent (calcium channels are likely involved) Lussitropy Coronaries: Minimal effect, less coronary vasodilation compared with Isoflurane Vascular Resistance: -ve Vasodilator |
| Respiratory Side Effects | Rate – Decreased Depth – Decreased Parenchymal effects: > Hypoxic pulmonary vasoconstriction inhibited > Bronchodilating |
| Central Nervous System Side Effects | ICP : Sevoflurane increases ICP between 0.5 and 1 MAC it isn’t huge. Seizure Threshold : non-epileptogenic Cerebral Vasodilatory Effects (hence ICP rise) CMRo2 depressed Nausea and vomiting Paediatric Emergence Delirium |
| Gastro-Intestinal Side Effects | nil |
| Metabolic/MSK: Side Effects | Potentiates NMB drugs |
| Obstetric | Uterine hypotonic |
| Toxicity Signs | Malignant Hyperthermia Trigger End point of volatile toxicity: CVS collapse Note in a toxic collapsed patient, your ability to get the vapours back out of the human is severely impaired…. as they require cardiac output to circulate and excrete agent via the lungs. The difference between anaesthetic dose and CVS collapse dose is wide…. and equipment and monitoring should stop you over doing it. But abroad under a bush with marauding rifle carrying individuals creates a different situation! |
Sevoflurane Pharmacokinetics
Sevoflurane undergoes 3–5% hepatic metabolism via CYP2E1, producing inorganic fluoride and HFIP (conjugated by glucuronide and renally excreted); 95–97% is eliminated unchanged via the lungs.
| Absorption | |
| Distribution | Extensively |
| Metabolism | Liver Phase I : 3-5% Deflurinated by the liver (CYP450 2E1) producing HexaFlourouIsoPropanol (HFIP) and inorganic fluoride ions. (CYP2E1 is induced ) Phase II : HFIP is rapidly conjugated with glucuronide and eliminated in urine. Alcohol excess, Phenobarbital, Smoking and Isoniazid use may induce p450 2E1 it is inhibited by Disulfiram- Induction of this enzyme may increase flouride concentrations, no evidence of toxicity ever having occurred |
Active Metabolites: Other Routes: | |
| Elimination | HFIP peak is at 12 hours. Elimination hl 55 hours 95-97% excreted via Lungs |
| Other Notable Information |
Strong Ion Difference and Lewis Acids?
We’ve gotten to grips with everything there is know about sevoflurane for the FRCA primary, but what on earth about Lewis Acids? this is more for general development of knowledge, and is an area that I have had to battle to marginal comprehend, I am no expert! Ultimately, it transpires that all the teaching on what an Acid is in the context of free hydrogen ions causing mischief is simplistic and devastatingly does not play out in reality. I am back at school again, being told that electrons in fact shift from the negative to the positive terminal in a battery (which I bet in itself is simplistic), having been lied to the previously that it was the other way around ‘because it was easier to explain’. As if a few years going by rendered my teenage brain capable of such transcendent shifts of comprehension.
During FRCA study there were rumblings of oddness, that the pressures of revision time availability laid to rest – why is water with carbon dioxide dissolved into it a weak acid? Why is sugar acidic and bad for your teeth?
If you want the full low down on this, naturally your best course of action is Deranged Physiology
Or check out this YouTube vid
An approximate historic journey would go
- Arrhenius’ lots of hydrogen ions = acid & lots of OH ions = base >>
- Bronsted Lowry definition of an acid is a molecule which can ‘loose its hydrogen atom’ and a base is a molecule that can pilfer a hydrogen from an acid molecule
- Lewis Acids a molecule that can either donate a proton or bind covalently with an electron pair.
Definitions Or Death
Strong Acid – One that is fully disassociated in solution to Hydrogen ion and conjugate base
Weak Acid – One that is partially disassociated in solution to Hydrogen ion and conjugate base
Strong Ion – An Ion that completely disassociates in a particular solution E.g
- Cations: Sodium / Potassium / Calcium / Magnesium
- Anions: Chloride
Strong Ion Difference (SID)- Is the difference between the concentrations of strong Cations/Anions [Na]+[K]+[Ca]+[Mg] – [Cl] + [L-Lactate]+[Urate] – or just Na – Cl
Much like anion gap, this number in normal physiology is not zero – as there are other elements like albumin that we dont look at as it its an ion! Chloride has significant potential to swing the SID. Hence why drowning Ms Miggens in 3 litres of Abnormal Saline 0.9% every day ends up with problems
Anion Gap – Not to be confused with the SID – calculation = (Na+ + K+) – (HCO3– + Cl–) [in hypoalbuminaemia you need to correct for the lower amount of negatively charged albumin floating about]
ATOT – the total of the non volatile weak acids in the solution
Lewis Acid –
IUPAC definition of lewis acid “: A molecular entity (and the corresponding chemical species) that is an electron-pair acceptor and therefore able to react with a Lewis base to form a Lewis adduct, by sharing the electron pair furnished by the Lewis base.
And then there is Stewarts theory? the headache continues!
This describes some clever (in my eyes anyway) maths that subsequently demonstrates that the controllers of Acid-base balance in a delightfully aqueous Human (not in some factory making things in all manners of different solutions) are:
- PACO2
- Strong Ion Difference
- Total non volatile weak acids in the system (ATOT / ATOT)
And that alterations in the above, influence Hydrogen ion and Bicarbonate concentrations to maintain electroneutrality of the system.
What this really ends up meaning is, the historic conflation of ph change and the bicarb change in a blood gas as the factors that influence one another – as per our usual teaching. But what we are really doing is measuring what we are seeing and assuming that must be the underlying mechanisms causing the H+ shifts.
This sodium chloride strong ion difference reality is what dictates the acidaemia triggered by accumulation of chloride in unwell patients, when they become hyperchloraemic the strong ion difference narrows and to maintain electroneutrality something has to shift and that must be to lessen the negatively charged bicarbonate floating about – leading to more H+ ions doing their hydrogen ion thing. Maintaining electroneutrality at the cost of a pH Shift towards acidaemia.
In reality when we slug 8.4% sodium bicarbonate into someone, we are handing them a load of sodium which alters the Strong Ion difference, and if were were to do the contrary with HCl the chloride is the SID shifting culprit.
References
- Water, strong ions, and weak ions, Chawla, Gunjan Drummond, Gordon et al. Continuing Education in Anaesthesia, Critical Care and Pain, Volume 8, Issue 3, 108 – 112
- Life in the Fast Lanes page on strong ion difference
- Deranged Physiology pages on Acid and Bases in Humans
- More Acid Base Fun this time a page from the physiology society that explains things pretty hacking well – Dr Jon-Emile S Kenny, Health Sciences North Research Institute and Flosonics Medical, Ontario, Canada
- An alternative approach to acid–base abnormalities in critically ill patients Badr, Adel et al. Continuing Education in Anaesthesia, Critical Care and Pain, Volume 7, Issue 4, 107 – 111
- L.I.G. Worthley, Strong Ion Difference: A New Paradigm or New Clothes for the Acid-Base Emperor, Critical Care and Resuscitation, Volume 1, Issue 2, 1999,
- Smith, M Nathanson, P F White, Sevoflurane–a long-awaited volatile anaesthetic., BJA: British Journal of Anaesthesia, Volume 76, Issue 3, Mar 1996, Pages 435–445, https://doi.org/10.1093/bja/76.3.435
- IUPAC LEWIS ACIDS
- Sevoflurane Lewis Acid Mis-behaviour
- Paediatric Emergence Delirium — BJA Education
Common questions
What is sevoflurane and why is it commonly used in UK anaesthetic practice?
Sevoflurane is a polyfluorinated isopropyl methyl ether volatile anaesthetic agent with molecular formula C4H3F7O. It is the most commonly used volatile anaesthetic in the UK due to its smooth non-irritant properties making it ideal for gas induction, reasonable onset and offset characteristics with a blood:gas solubility coefficient of 0.69, and the lowest global warming potential compared to other volatile agents like desflurane and isoflurane. It has a MAC value of 2.0% in adults (1.8% at 40 years) and boiling point of 58.6°C with a saturated vapour pressure of 22.7 kPa at 20°C.
What are the cardiovascular effects of sevoflurane?
Sevoflurane produces dose-dependent negative inotropic effects, likely through calcium channel interaction, and causes peripheral vasodilation leading to decreased vascular resistance. It has minimal effect on heart rate (chronotropy) and less coronary vasodilation compared with isoflurane. The cardiovascular depression is generally well-tolerated in healthy patients but requires consideration in patients with compromised cardiac function. The agent maintains a wide margin between anaesthetic dose and cardiovascular collapse.
How is sevoflurane metabolized and eliminated from the body?
Sevoflurane undergoes minimal metabolism with only 3-5% metabolised by the liver via cytochrome P450 2E1. Phase I metabolism produces hexafluoroisopropanol (HFIP) and inorganic fluoride ions through defluorination. Phase II metabolism involves rapid conjugation of HFIP with glucuronide for urinary elimination, with HFIP peak levels at 12 hours and elimination half-life of 55 hours. The majority (95-97%) is eliminated unchanged via the lungs. CYP2E1 can be induced by alcohol, phenobarbital, smoking, and isoniazid, potentially increasing fluoride concentrations, though no evidence of fluoride toxicity has been documented.
What are the respiratory effects of sevoflurane?
Sevoflurane causes respiratory depression by decreasing both respiratory rate and tidal volume in a dose-dependent manner. It inhibits hypoxic pulmonary vasoconstriction, which may affect ventilation-perfusion matching in patients with lung pathology. Sevoflurane produces bronchodilation, making it useful in patients with reactive airways disease. Its non-irritant properties on the airway make it the preferred volatile agent for gas induction, particularly in paediatric anaesthesia.
What are the potential complications and degradation products of sevoflurane?
Sevoflurane can degrade via two pathways: interaction with warm desiccated alkaline CO2 absorbers at low fresh gas flows produces Compound A (pentafluoroisopropenyl fluoromethyl ether) and Compound B, plus formaldehyde and methanol derivatives (Compounds C, D, E). These compounds are potentially toxic but never reach toxic concentrations clinically. Sevoflurane is a malignant hyperthermia trigger. It increases intracranial pressure between 0.5-1 MAC through cerebral vasodilation. Paediatric emergence delirium is a recognised complication. The formulation contains 300 ppm water to prevent degradation and hydrofluoric acid formation that occurred with older anhydrous preparations.
What is the MAC value of sevoflurane and what does this mean clinically?
Sevoflurane has a minimum alveolar concentration (MAC) of 2.0% in adults (decreasing with age to approximately 1.8% at 40 years), which represents the alveolar concentration at which 50% of patients do not move in response to surgical stimulation at 1 atmosphere. MAC is used to compare potency between volatile agents and guide clinical dosing. The blood:gas solubility coefficient of 0.69 indicates relatively rapid onset and offset characteristics. In clinical practice, sevoflurane is typically administered at 0.5-2 MAC depending on the clinical scenario, patient factors, and use of adjuvant agents. The oil:gas solubility coefficient of 47 correlates with its anaesthetic potency.
Thanks for listening. Take it day by day, don't overcook yourself — keep studying.
Transcript
32 min listenRead the full transcript
Introduction and Welcome
00:00–00:42
Hello, and welcome to Gas, Gas, Gas. This is the best podcast for the FRCA primary exam. Our goal is to fill your brain with all this highly useful information. You might be in the gym right now, commuting, or ironing your scrubs. Regardless, the revision is eventually going to end, but for now, expect facts, concepts, model answers, and the odd tangent. Make sure to check out gasgasgas.uk. There’s show notes there, there’s loads more detail. Make sure to like and subscribe. Anyway, buckle up, get ready for your mind to be bent into a new shape, and let’s get on with the show.
Episode Overview: Why Study Sevoflurane?
00:34–03:12
Key Points:
- Sevoflurane is commonly used, so examiners expect detailed knowledge
- Important for compare/contrast questions with other volatile agents
- SBA questions often test knowledge of boiling points, blood-gas solubility, and MAC values
- Understanding relative properties helps navigate exam questions
Hello everyone, and welcome to Gas, Gas, Gas. This episode handles sevoflurane for the FRCA primary exam. Now you’re probably thinking, oh, what do I need to know about sevoflurane? I’ve used that all the time. Why bother listening? And there’s a number of things that you’re going to learn.
When we go through sevoflurane, a few things that I certainly didn’t know and would be quite fun to talk about in an exam, but I think it would be pretty criminal to talk to you about in an exam. But we just roll back to the reality that is something that is used commonly, they’re going to want you to know a lot about it. If you could just say morphine’s a great pain-relieving drug, they’re not going to be like, oh yeah, great, he knows what he’s on about. If you use morphine every day, the expectation is that you really know the ins and outs of that drug, and the potential misbehaviour that might happen very rarely, but if you use it a thousand times, then it’s not so rare.
One of the things we’re going to talk about is sevoflurane. There’s always going to be scope for asking you to compare and contrast these agents, and you need some sort of structure in the viva with which to hang that on. And in SBAs they’re going to try and catch you out in making you weigh up where desflurane, isoflurane, and sevoflurane sit within one another in terms of blood-gas solubility or boiling point and all that madness.
Now, in terms of sevoflurane as a clinically used volatile anaesthetic agent, I’m sure we’ve all used it. It is a volatile anaesthetic drug. It has likely the least offensive global warming potential, and has reasonable onset and offset times. We know that desflurane might be a winner on onset and offset. However, polar bears are exceedingly allergic to desflurane, and I think there’s quite a few penguins looking around large walk-in freezers perhaps due in part to the use of desflurane.
There’s other episodes in the series that talk about how volatiles behave in a human being and how to utilise them. But I certainly reflect back to one of the very first anaesthetics I did by myself, where I was absolutely terrified of that MAC number not being enough. If you were to plot my anaesthetic volatile anaesthetic dose over time, it was probably like traversing the Himalayas in terms of the peaks and troughs, because I didn’t want to overdose them. Oh, but I don’t want to underdose them. I didn’t really truly comprehend how these things behaved.
Check out the compartmentalised volatile anaesthetics episode. It’s quite early on in the podcast if you’ve not listened to it. That explores how these agents behave within the anaesthetic circuits and the humans that we attach those anaesthetic circuits to.
Anyway, that’s lots of talking. We’re going to get into the nitty-gritty of sevoflurane and everything you need to know to handle the SBA and the SOE viva joys that you’re all so looking forward to doing.
Classification and History
03:12–04:37
Key Points:
- Polyfluorinated isopropyl methyl ether with seven fluorine atoms
- First synthesised in 1960 (same time as isoflurane)
- Took longer to reach market due to more challenging manufacturing
- Approved in Japan (1990), then US as Ultane (1995)
- Generic versions available from 2006
Right, sevoflurane. You’ve got to have a classification for this drug. You could call it a volatile anaesthetic agent, and that will probably get you most of the way in the exam. But if we’re being particular, it is a polyfluorinated isopropyl methyl ether. What does it mean by polyfluorinated? Well, that means that it’s got lots of fluorines. It’s called sevoflurane—sevo, seven. There are seven fluorines in sevoflurane.
What about some history before we really dive deep? So it was first synthesised in 1960, which is pretty much the same time as isoflurane. However, isoflurane was much easier to make, and that’s why isoflurane kind of took the mantle and was the volatile anaesthetic agent of choice for quite some time. Sevoflurane seemingly sat on a shelf. Its production rights were then sold to a company called Maruishi Pharmaceuticals, who brought sevoflurane to market in Japan in 1990. And then Abbott Pharma in 1995 branded it as Ultane, and it became available. Generics of sevoflurane were actually only available from 2006.
Why did it take longer to get to market? Well, manufacturing sevoflurane was trickier. Getting the fluorines attached was more challenging. Isoflurane had really come about courtesy of the much-improved chemistry around fluorine that was built upon during the Manhattan Project of all things. But everyone picked the easy one to take to market. But now, of course, I bet you nine times out of ten you’re going to pick sevoflurane over isoflurane.
Is it an isomer? No, it’s not.
Physical and Chemical Properties
04:38–05:00
Key Points:
- Appearance: clear, colourless liquid
- Non-flammable
- Stored in plastic containers
- Not an isomer
How does it appear? It is a clear, colourless liquid, and it is non-flammable, and it’s stored in plastic containers.
Stability and Chemical Reactions
05:00–07:59
Key Points:
- Forms compounds A, B, C, D, and E in warm, dry, alkaline CO₂ absorbers at low fresh gas flows
- Requires moisture (water content) to prevent hydrofluoric acid formation
- Original preparations: 100 ppm water; current preparations: 300 ppm water
- Can react with Lewis acids (glass, aluminium) when dry
- UK practice: low-flow anaesthesia is standard; US practice: higher fresh gas flows due to compound concerns
How stable is sevoflurane? So there is some mischief that sevoflurane can get up to. In warm, dry, alkaline CO₂ absorbers at low fresh gas flows, it can produce a number of compounds that can cause bother. These are often labelled compounds A, B, C, D, and E. A and B are the initial compounds formed, and then subsequently C, D and E conform from these.
There’s lots of hesitancy about low-flow anaesthesia with sevoflurane. In the UK, we just get on with it and go down to however many millilitres of oxygen the patient requires, plus countering any circuit leaks. As I understand it, in the US and some places, they run quite high fresh gas flows when using sevoflurane because of their terror of these compounds. Again, this is perhaps an example of dogma in either direction. Perhaps we’re wrong. Perhaps we’re not. Perhaps the folks in the United States are playing it safer. Or maybe the sevoflurane lobby is saying, oh, you must use lots of sevoflurane, then we’ll make more profit. Who knows?
Now, interestingly, and there’s a link in the show notes, sevoflurane needs moisture. And when I say moisture, it needs water dissolved into this volatile anaesthetic liquid. If there is no water in your sevoflurane, sevoflurane has a much greater potential of causing quite significant mischief. This is one of the reasons why it’s stored in a plastic bottle, and why vaporisers are made of certain materials.
If you are using a glass bottle with dry sevoflurane or a metallic bottle, or perhaps a vaporiser with certain metals such as aluminium—remember, aluminium forms an oxidated layer on its external surface, otherwise it’s very reactive—these storage materials behave like Lewis acids. And you’re probably thinking, what on earth is a Lewis acid? And I also thought that. I’ll have to find it a bit later in the episode. But if there’s any people who’ve done chemical engineering before medicine, and they think, you know what, I could explain Lewis acids, great, email me and we’ll get you on the show and you can have your ten minutes of explanatory fame and we’d all appreciate it.
But anyway, these materials that either pipe the sevoflurane to the patient or store the sevoflurane contain Lewis acids. Sevoflurane, when it’s making friends with Lewis acids, converts to hydrofluoric acid. You’re right, that does sound like a problem, and it has been a problem, and actually vaporisers have been altered, having previously been noted to be damaged by sevoflurane. This can be entirely mitigated by making sevoflurane sufficiently wet. I think original preparations had a water content of 100 parts per million. Today’s sevoflurane generally has 300 parts per million. But remember it’s a generic now, lots of people could manufacture it. Let’s hope they stick to those robust standards.
I don’t think there’s been any evidence of patient harm, but there was a big hoo-ha that led to changing vaporisers, making sure sevoflurane was moist enough, that came about as these products were brought to market by different people. When I say people, I mean companies. Anyway, that’s crazy, isn’t it?
So sevoflurane, whilst seemingly quite stable, isn’t completely stable. In the exam, just mention compounds A, B, C, D and E. They ain’t going to ask you about Lewis acid hydrofluoric misbehaviour. That’s just an interesting niche. So generally speaking, these compounds A, B, C, D and E interact with soda lime when it gets quite warm, up to like 65 degrees C. These are potentially toxic agents, however, they never reach toxic concentrations.
Physicochemical Properties: Key Numbers
08:11–10:54
Key Points:
- Molecular weight: 200 g/mol
- Boiling point: 58.6°C
- Saturated vapour pressure (SVP) at 20°C: 22.7 kPa (≈22% at equilibrium)
- MAC: 1.8–2.2% (age-adjusted; aim for 2% in younger patients)
- Blood-gas solubility: 0.69 (compare: desflurane 0.45, isoflurane 1.4)
- Oil-gas solubility: 47 (compare: desflurane 26, isoflurane 98)
- Sevoflurane is approximately half as soluble as isoflurane
- Sevoflurane is approximately half as potent as isoflurane
Molecular weight: get your pens and papers, 200 grams per mole, which is actually a very nice, neat number. What does sevoflurane boil at? 58.6 degrees—that is not a convenient number, but it boils at 58.6.
Its saturated vapour pressure at 20 degrees C—remember, it’s always quoted at 20 degrees C—is 22.7 kilopascals. SVP, think about it like this, guys. If you pour some sevoflurane into a container, put the lid on, let it equilibrate, the partial pressure of sevoflurane in that container will eventually end up being 22.7 kilopascals if you have it at 20 degrees. If you then were to take a long haul from your container, that’s the sort of equivalent of getting 22% sevoflurane, isn’t it?
Now, one lungful, 500 millilitres, probably isn’t enough to be completely harmful, but you might get a very, very, very high plasma concentration initially, which, you know, probably will tank your blood pressure and render you briefly unconscious until it re-equilibrates. I thoroughly wouldn’t recommend that.
So saturated vapour pressure sevoflurane: 22.7.
The MAC of sevoflurane, which is the relevant next step to talk about, is 1.8%, although you might see 1.8 to 2.2%. Remember, MAC is age-adjusted. If in doubt with a relatively young person, you could aim for 2%. I’m not going to talk about all the different variants of MAC here. That’s for another episode which has already happened. There’s a link in the show notes to that episode.
Blood-gas solubility coefficient of sevoflurane is 0.69. Remember that the blood-gas solubility of isoflurane is 1.4 and desflurane is 0.45. Remember these are on a spectrum, so 0.45 desflurane, 0.69 sevoflurane, 1.4 isoflurane. So approximately, isoflurane is three times more soluble than desflurane. Sevoflurane is pretty much half as soluble as isoflurane—0.4 to 0.69, 0.69 to 0.7. So in an exam where they’re trying to make you think which one is approximately less or more soluble, you can sort of remember those halves there.
What is the oil-gas solubility coefficient? Remember, oil-gas dictates potency of agent. Drugs with a lower MAC likely are more potent, and the oil-gas solubility coefficient for sevoflurane is 47. Desflurane is 26. And remember the MAC of desflurane is 6.6, so you need a lot more desflurane to keep someone the same amount of anaesthetised.
Seemingly, sevoflurane and isoflurane, very conveniently, the oil-gas solubility for isoflurane is 98, which is kind of double. So you can, in your head, think: well, isoflurane is about twice as potent as sevoflurane, but sevoflurane is half the solubility of isoflurane. So that frame in your mind might help you in the exam when talking about comparing these drugs.
So those are some of the physicochemical properties.
Pharmacodynamics: Mechanism of Action
10:57–12:16
Key Points:
- Acts primarily on GABA-A receptors (ionotropic receptors)
- Facilitates chloride ion influx, causing hyperpolarisation
- Also affects NMDA receptors and potassium channels
- Different volatile agents have varying receptor profiles (e.g., methoxyflurane for analgesia)
Going to move on to pharmacodynamics of sevoflurane now. How do volatile anaesthetic agents work? We know that they act on proteins, chiefly GABA-A proteins. When I say proteins, we’re talking about structures on cell membranes that exert effects on that cell when you alter those structures by binding to them.
GABA-A receptors—these are ionotropic receptors that generally speaking let in chloride ions when they’re open. Volatile anaesthetic agents facilitate GABA-A receptors to be more likely to be open, therefore hyperpolarising cells, making transmission less effective. There are some suggestions that volatile anaesthetic agents also work on NMDA receptors as well as potassium channels. Now some agents behave more like this than others.
So remember, we’re giving folks Penthox in A&E for their smashed up femurs. Penthox is a volatile anaesthetic agent that we use to treat pain. Therefore, presumably it must exert an effect on receptors that modulate pain, either directly or through a chain of effects that leads to alterations in how other receptors work. But we’ll do an episode on Penthox or methoxyflurane later in the volatile anaesthetics chapter.
Pharmacodynamics: Effects on Organ Systems
12:16–16:20
Key Points:
Cardiovascular:
- Minimal effect on heart rate
- Negative inotropic effect (reduces myocardial contractility)
- No data on dromotropy (AV nodal conductivity) or lusitropy (relaxation capacity)
- Excellent bathmotropic stability (doesn’t alter myocardial excitability, unlike halothane)
- Minimal coronary artery effects (less vasodilation than isoflurane)
- Dose-dependent reduction in systemic vascular resistance (SVR)
Respiratory:
- Reduces respiratory rate and tidal volume
- Central nervous system-mediated respiratory depression
- Inhibits hypoxic pulmonary vasoconstriction (HPV) – can worsen V/Q mismatch in COPD
- Bronchodilation – useful in bronchospasm (can be used in ITU for severe cases)
Central Nervous System:
- Hypnotic, amnestic, and immobilising effects
- Minimal effect on intracranial pressure within therapeutic range
- No effect on seizure threshold
- Cerebral vasodilation
- Reduces cerebral oxygen consumption
- Causes nausea and vomiting
- Emergence delirium in children – severe disorientation, inconsolable distress; treated with dexmedetomidine, clonidine, or propofol
Other Systems:
- No significant GI or metabolic effects
- Obstetric: causes uterine hypotonia (increased bleeding risk)
Toxicity:
- Trigger for malignant hyperthermia
- Overdose endpoint: cardiovascular collapse
- Wide therapeutic window, but avoid accidental high concentrations (e.g., 8% at 15 L/min flow)
So, pharmacodynamics, guys, remember, is about what the drug does to the person, as opposed to what the person does to the drug. Mechanism is one element of that, and then side effect profile is the other. And you could argue that chief effect needs to be in this. But we all know that its chief effect is to render someone hypnotised and amnesic and generally less mobile.
Side effect profile of sevoflurane, we know. So sevoflurane is pretty stable, isn’t it? We’ve had lots of drugs in the past, like halothane and all those explosive agents and ether and ethylene, which were much less well tolerated by humans. Here we are, as anaesthetists, in the 21st century, living it up with sevoflurane.
What are the cardiovascular effects of sevoflurane? So it doesn’t really mess with your heart rate. From an inotropic perspective, it has a negative effect. So it does lead to less contractility in your myocardium. Does it alter your dromotropy or your lusitropy? Remember, these are AV nodal conductivity and capacity to relax respectively. There’s no data. What about bathmotropy? Sevoflurane is really stable. It doesn’t alter myocardial excitability, unlike halothane. Coronary arteries, minimal effect on those. You see less coronary vasodilation compared with isoflurane, and as you might expect, it lowers your vascular resistance. It drops your SVR in a dose-dependent manner.
What about the respiratory system? So, I’m sure we’ve seen patients who have some sevoflurane and they are less interested in breathing. Now, you could make an argument that this is a respiratory side effect mediated by the central nervous system side effect of sevoflurane, but it’s better to stick it in respiratory. So you get a reduction in the rate of breathing and the depth of breathing.
What are the parenchymal effects of sevoflurane—i.e., actually direct effects on the lungs? So it inhibits hypoxic pulmonary vasoconstriction. You might be thinking, ah, that’s great. That means that there’s more blood flow to the lungs, but it also means there’s more blood flow to bits of the lungs that are harder to ventilate. So we’ve got someone with COPD and their lungs are pretty knackered. You’re then basically causing yourself to end up with a shunt where there’s blood flow across bits of the lungs that you really can’t get at. But it is also usefully bronchodilating. So you might get a degree of balance against that problem.
But sevoflurane is useful in ITU, in extremis, where you can administer a volatile agent to someone who is in a rip-roaring bronchospasm and has been for days. And if you’re doing a TIVA anaesthetic and someone gets all bronchospastic, you definitely should stick some sevoflurane on, alongside all your other therapies, I would say. Make your life easier.
Central nervous system effects. So, obviously, we’ve spoken that it’s hypnotising, it renders you unable to form memories, it makes you less responsive to pain stimuli and flattens your spinal cord’s reflexes to being jabbed. Within the therapeutic range of sevoflurane, it doesn’t tend to influence intracranial pressure too much, but it certainly does have an effect—hence why neuroanaesthetists prefer, generally speaking, TIVA these days. It doesn’t alter seizure threshold. As you can expect, it does cause cerebral vasodilation because it vasodilates everywhere else. It reduces the amount of oxygen your brain consumes, and it causes nausea and vomiting.
Of particular interest from a CNS side effect perspective: in children, kiddies tend to get an emergence delirium, and they are completely inconsolable, distressed, disorientated, have no idea what they are, who they are, when they are, and really they’re very challenging and they just eventually snap out of it. But it can be very distressing for recovery staff and parents trying to console them because they’re literally completely batty. Dexmedetomidine, clonidine helps, and if you give a dose of propofol as you’re waking them up, it sort of smooths things out. Who knows why?
There aren’t any particular GI or metabolic side effects. From an obstetrics perspective, as with all volatile anaesthetic agents that are in use today, it causes a hypotonic, floppy uterus, which means more bleeding. Toxicity-wise, it is a trigger for malignant hyperthermia and you can overdose someone on sevoflurane, and that endpoint is cardiovascular collapse. Very hard to get there because the therapeutic window is really wide, but certainly you can overdose this drug. Do not accidentally leave the vaporiser on 8% with flows of 15 litres per minute. You’ll just absolutely hose in and fill that patient with sevoflurane, which is then more challenging to get out if their blood pressure is five.
Pharmacokinetics
16:20–18:49
Key Points:
- Distribution: Extensive (quite soluble, enters multiple compartments)
- Metabolism: 3–5% metabolised by liver via CYP2E1 pathway
- Compare: isoflurane only 0.2% metabolised
- Produces hexafluoroisopropanol (HFIP) and inorganic fluoride ions
- CYP2E1 inducers (increase metabolism): smoking, alcohol excess, phenobarbital, isoniazid
- CYP2E1 inhibitor: disulfiram
- Elimination: 95–97% excreted unchanged via lungs
- HFIP peak at 12 hours, elimination half-life 55 hours (non-toxic concentrations)
- Clinical relevance: Smokers may require higher doses to maintain end-tidal concentration, but MAC targeting prevents awareness
Okay, pharmacokinetics of sevoflurane. Remember, pharmacokinetics is what the body does to the drug. I could not tell you what the first-pass metabolism of sevoflurane is. I don’t think we’ve got anyone to drink it to find out. I don’t know how palatable it is. Its distribution is extensive. It is quite soluble, isn’t it? It will get into all these compartments. I don’t think there’s a quoted volume of distribution here, so I wouldn’t worry too much.
The real money in kinetics is metabolism, and sevoflurane is 3 to 5% metabolised by the liver. Remember isoflurane is barely metabolised at 0.2% for isoflurane. So a fair bit of metabolic action occurs with sevoflurane. It is your CYP2E1 pathway, generally speaking, and it produces HFIP and inorganic fluoride ions. HFIP—hexafluoroisopropanol. You don’t need to know that for the exam, unless someone’s being terribly, terribly, terribly mean. You don’t need to know that bit. But 3 to 5% metabolised by the liver by a cytochrome pathway, yes.
Why? Because you can induce CYP2E1, for example, in smokers. That means they’re going to get through more sevoflurane, which means that your dose of sevoflurane has to be up. Your MAC is generally still okay, because remember, MAC is utilising your end-tidal fraction of agent, and that is presumed to align with the fraction of agent in the brain, as opposed to the fraction of agent being metabolised. So as long as you’re targeting your end-tidal volatile anaesthetic agent to the right amount, you’re unlikely to have any greater incidence of awareness. They might recover just a smidge quicker. Great, but you might need to administer more agent to keep them where they need to be.
There are a few other things that induce it. Alcohol excess can induce and improve sevoflurane clearance, alongside phenobarbital—that’s a drug used for seizures that isn’t used very much at all these days, but you might have the odd, unusual 80-year-old who just is on it—and isoniazid. But, you know, not such a common drug. And interestingly, you can inhibit CYP2E1 with disulfiram, which is that drug you can use to make people feel really awful if they have an alcoholic drink.
Elimination: 95 to 97% is excreted via the lungs, unchanged. That HFIP, its peak is at 12 hours and its elimination half-life is 55 hours. But remember, we’re really not hitting anything that could be mistaken for a toxic concentration here.
If you can get most of that in your brain, you’ll be laughing for the exam.
Reflections on Anaesthetic Safety
18:49–20:36
Key Points:
- Modern anaesthesia is remarkably safe due to extensive refinement
- Historical challenges: explosion risks, special footwear, humidity control
- Public perception of anaesthesia as dangerous persists despite safety improvements
- The “normalisation” of anaesthesia can make us lose sight of how remarkable modern practice is
And I just want to reflect, before we go into the sort of semi-educational chunk of this episode, on this sevoflurane Lewis acid stuff. And I just realised that we use this drug, and I was certainly using this drug, with absolutely no idea about the fact that there was water in it, and that the water was there to basically stop the sevoflurane, which is a relatively stable, innocuous, seemingly volatile anaesthetic agent that doesn’t explode, from starting to eat its way out of a vaporiser slowly but surely.
And it just reminds me that anaesthesia has come really, really, really far and is very, very, very safe, and we don’t realise all the effort that has gone into achieving safe anaesthesia practice in the world. And I just find it a bit mind-blowing that our colleagues of old used to tolerate a mild risk of explosions, having to wear anti-static footwear and fixing humidity in theatres to avoid fires and blown-up patients.
But I suppose the hangover from all these events is the public’s perception of anaesthesia being terrifying, scary, risky, dangerous, when actually most of the time it was far more dangerous to drive to the hospital in the first place. But people are always seemingly far more terrified of the anaesthetic than the fact that there’s going to be a surgeon rearranging bits of them, and I’m always quite perplexed by that.
But then, here we stand, anaesthetising people day in, day out. We’re quite used to it, it’s quite normalised to us. And it’s very easy to lose the insight into the fact that it is absolutely barking mad that we are allowed to take a load of drugs that in any other hands would probably be quite lethal, administer them in a sensible manner, rendering someone completely incapable of defending themselves from a surgeon, and then them having their operation, and then us waking them up, saying, well done, you did great. Take some breaths. Out comes the tube. Bonkers. Absolutely great job.
So remember, guys, just keep studying. It is worth it. It is cool.
Educational Deep Dive: Lewis Acids, Acid-Base Chemistry, and Strong Ion Difference
20:36–29:03
Key Points:
Lewis Acids:
- A molecule that can donate a proton OR bind covalently with a free electron pair
- Example: ammonia (NH₃, base) and ammonium (NH₄⁺, acid) equilibrium
- Relevant to sevoflurane’s interaction with certain storage materials
Acid-Base Definitions:
- Arrhenius: Acid = lots of H⁺ ions; Base = lots of OH⁻ ions
- Brønsted-Lowry: Acid = molecule that loses hydrogen; Base = molecule that accepts hydrogen
- Lewis: Acid = electron pair acceptor; Base = electron pair donor
Strong Ions:
- Ions that completely dissociate in solution (e.g., Na⁺, Cl⁻, K⁺, Ca²⁺, Mg²⁺, lactate, urate)
- Unlike weak acids (e.g., CO₂/H₂O reactions, vinegar)
Strong Ion Difference (SID):
- Calculation: [sum of positive ions] − [sum of negative ions]
- Simplified: [Na⁺] − [Cl⁻]
- Normal value: 42 (compare anion gap: 4–12)
- Note: Unlike anion gap, which uses Na⁺, K⁺, HCO₃⁻, Cl⁻
Stewart’s Theory:
- Proposes that acid-base balance is determined by:
- CO₂ concentration
- Strong ion difference
- Total non-volatile weak acids (Atot)
- Suggests pH and bicarbonate are effects rather than causes of acid-base changes
- Explains hyperchloraemic acidosis from normal saline better than traditional Henderson-Hasselbalch approach
- Sodium bicarbonate works by providing excess strong ions (Na⁺) with low Cl⁻, shifting pH towards alkalotic
- More complex than traditional pH/bicarbonate understanding; pH/bicarbonate remains clinically practical
Clinical Relevance:
- Unlikely to be examined in detail
- Useful for understanding ITU consultants’ discussions
- Helps explain mechanisms behind fluid resuscitation choices
Now, what on earth is a Lewis acid? Well, this is a question I’ve asked myself, and I’m still not entirely convinced I know the answer. There are resources on the internet—there’s a Khan Academy video on it. There’s a Deranged Physiology chapter delight on Lewis acids, but also a few other important things about pH in a human. And I’d be very surprised if Lewis acids or strong ion difference came up in the exam. I think strong ion difference is probably a viva sort of conversation. But I’m including it A for my own educational benefit, B, because I’ve heard it mentioned loads of times at work and I’ve just thought I have no idea. And C, because hopefully you might have a modicum of a Scooby-Doo if it is mentioned at work and might be able to extract some useful teaching from someone who understands it more effectively, and therefore we’ll all start to learn about it and understand it better.
Why am I interested in this? Well, ultimately it transpires that perhaps our rudimentary perception of what an acid is is not entirely placed in reality. And it just takes me back to my GCSE science days where teachers before then had told me that electrons moved from the positive end of a battery to the negative, and then the next year, when it was deemed that your brain was capable of understanding such complicated and challenging things, they deigned to say, well, actually, I know electrons are negative and they come from the negative terminal, actually, but they don’t really quite move in the way we told you either. And that just infuriates me.
Why open with something that is a load of nonsense when we’re all capable of appreciating something that’s hard to understand but real as opposed to something that is entirely simplistic? But I’m going to say it is much easier to think about pH in the way we think about it with Henderson-Hasselbalch than any of this other stuff.
So generally speaking, there’s been a journey of what an acid is over time. There was someone called Arrhenius, and he said that if there are a lot of hydrogen ions in a beaker, it’s an acid, and if there are a lot of OH⁻ hydroxyl ions, then it’s a base. Brønsted and Lowry came out saying an acid is a molecule which can lose its hydrogen atom. So we’re calling the molecule an acid as opposed to the hydrogen ion mass an acid. And a base is a molecule that can pilfer a hydrogen from an acidic molecule.
But now, what on earth is a Lewis acid? So there’s an IUPAC definition—this IUPAC is like an international collaboration that defines chemical concepts so that chemical engineering can happen effectively—but a Lewis acid, as defined by them, is a molecular entity that is an electron pair acceptor and therefore able to react with a Lewis base by sharing said electron pair furnished by said Lewis base. And I read that and thought, ah, that makes no sense to me whatsoever. And it probably doesn’t make much sense to you either.
So to distil it down, a Lewis acid is a molecule that can either donate a proton to a system or bind covalently with an electron pair that’s free and available within that system. So, an example that we might have come across is ammonia and ammonium. Our NH₃ is a base and it’s got some spare electrons on it. And our NH₄⁺ is an acid, and actually it ends up slightly positively charged. When you introduce a hydrogen ion to the situation, NH₃ plus a hydrogen ion leaves you with NH₄⁺. And here we have a system that equilibrates, doesn’t it?
Much like your CO₂-H₂O-carbonic anhydrase-carbonic acid reactions that occur throughout the human, we know that how much forms a hydrogen ion versus a bicarbonate is dependent on the environment it is in. Why are we interested in Lewis acids and bases? Well, it opens up more broadly to things that could behave in a slightly acidic manner that the Brønsted-Lowry vibe might not tie in with directly. And that’s why you get some weird Lewis acid action with sevoflurane when it’s experiencing an introduction to either slightly metallic materials or glass-like materials, whereby we’ve got some molecules that would accept some electrons and therefore you can trigger inadvertent reactions. Ultimately, don’t worry about Lewis acids too much.
What about strong ion difference? Now, this is something that is actually something more applicable in reality. I’m just going to smash through some definitions of acidic things quickly, because this certainly can come up in an exam. Remember, a strong acid is defined as one that is fully dissociated in solution. And when we say solution, for the sake of human beings, this is an aqueous solution. We are watery things. Strong acids fully dissociate into their hydrogen ion and their conjugate base—hydrofluoric acid, hydrochloric acid, etc.
A weak acid is one that is partially dissociated in solution to a hydrogen ion and its conjugate base, and you’re best off thinking about your CO₂-water type reactions for this, or vinegar. That’s a weak acid.
So, what is a strong ion? The important word here is ion. This is an ion that completely dissociates in a particular solution. So remember, when dry, sodium chloride forms a crystalline structure of a sodium and a chloride atom. Chuck that in water, it dissociates, and then you’ve got some sodiums floating around quite happily, and some chloride ions floating around quite happily. Thus, sodium and chloride are strong ions. Other strong ions you find in a human: potassium, calcium, magnesium, and then also urate and lactate.
How do you calculate the strong ion difference? A bit like the anion gap—we’re going to define that in a second—you add your concentrations of all the positives to the sum of all the negatives and subtract the negatives from the positives. So that would be your concentrations of sodium, potassium, calcium, magnesium minus your chloride, lactate and urate. But in reality, most people just go for a simplified sodium minus the chloride.
Now much like anion gap—and remember the anion gap is different; it takes into account sodium and potassium as the positives and bicarbonate and chloride as the negatives—both strong ion difference and anion gap don’t measure out to zero in humans, i.e., there are some negative molecules that we do not account for. A normal strong ion difference is 42, which is a great number, isn’t it? We all like 42, meaning of life. Whereas anion gap is normally 4 to 12.
But why do we actually care about strong ion difference? Well, we have a theory, and it’s Stewart’s theory, and the headache does indeed continue. Stewart’s theory describes some, in my eyes anyway, clever maths that demonstrate that the things that control the acid-base balance in a delightfully watery human is not your pH and your bicarbonate. I mean, I almost fell off my seat, but actually, it is determined by your CO₂ concentration, your strong ion difference, and the total non-volatile weak acids in the system described as A subscript total.
Now, why can’t we just stick with pH and bicarbonate? Well, ultimately, we do. And the reality of it is that it was much easier to measure pH and bicarbonate, and us as humans have probably stumbled forth and conflated bicarbonate and pH changes as the things that directly dictate the alterations in pH in a human, when in fact actually other things were going on, but the net effect was that we saw changes in pH and bicarbonate. So it’s kind of like we’ve measured it, so that must be the mechanism that’s happening, instead of measuring it and really knowing that something else was occurring underneath.
And this goes some way to describing these hyperchloraemic problems we see with giving someone too much normal saline. So, in reality, for example, if we have skipped past that normal saline, but we’ve reached for a bottle of 8.4% sodium bicarbonate and we’re trying to fix someone because they’re just too acidic, we’ve given them the sodium bicarbonate and we’ve handed them a load of strong ion, and this excess of sodium with a paucity of chloride tips their pH back towards being alkalotic. And then we have the bicarbonate, which ultimately swaps out to being CO₂, which you can blow off.
This would suggest that there’s more going on under the hood than we perhaps are taught to realise. And in reality, does it make a tremendously large difference most of the time? Not really. And pH and bicarbonate is easier to understand. There’s going to be some links in the show notes to some BJA articles that go into it in more detail, and I can only hope that they would bolster your understanding of this.
I think the most important thing is to just have some robust definitions of what these are so that you have an approximate appreciation in order to understand what the ITU consultant starts talking about when they get carried away. I just thought it was interesting because sevoflurane turned to hydrofluoric acid and caused mischief. That’s cool.
Closing Remarks
29:03–30:06
Anyway, thank you very much for listening, guys. I hope you have a delightful weekend. The next episode is going to be on desflurane, I do believe. And then we’ll probably handle halothane, probably methoxyflurane. And then we might explore some of the slightly weirder stuff, looking at the sort of history of volatiles slightly with ether, and perhaps talk about explosions. Because I do think there’s an e-learning for health chapter on explosions. And I’ve got a book entitled Physics for Anaesthetists with a chapter on explosions which I’ve found in a charity shop that I’ve been meaning to read for ages, so I will have the luxury of reading that.
Have a nice weekend. Thank you very much, folks. Don’t forget to like and subscribe. Cheerio!
Enjoyed this? Review on Apple Podcasts Rate on Spotify
Support the show Help keep the lights on SBA question bank @ Teach Me Anaesthetics